-
Welcome to Celiac.com!
You have found your celiac tribe! Join us and ask questions in our forum, share your story, and connect with others.
-
Celiac.com Sponsor (A1):
Celiac.com Sponsor (A1-M):
-
Get Celiac.com Updates:Support Celiac.com!
Search the Community
Showing results for tags 'malabsorption'.
Found 13 results
-

 Celiac.com 01/27/2024 - We've done many articles that cover nutrient deficiencies that are associated with untreated celiac disease, but many people do not realize that celiac disease can also lead to malabsorption of medications and supplements. Celiac disease damages the lining of the small intestine, where both nutrient and certain medication absorption takes place. This damage can result in decreased absorption of various substances, including both over the counter and prescription medications, and supplements. Medications that are taken orally and absorbed in the small intestine may be affected by malabsorption in individuals with untreated celiac disease. As a result, the effectiveness of these medications might be compromised. It's essential for individuals with celiac disease to maintain a strict gluten-free diet to allow the small intestine to heal and improve nutrient absorption, including medications. Common Medications Affected by Celiac Disease Malabsorption Here are some common medications that may be affected by celiac disease-related malabsorption, but many more medications might also be affected: Thyroid Medications: Medications used to treat thyroid disorders, such as levothyroxine, may have reduced absorption in individuals with untreated celiac disease. Certain Antibiotics: Some antibiotics, including tetracycline and doxycycline, are absorbed in the small intestine. Malabsorption issues may affect their effectiveness. Anti-Inflammatory Drugs: Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen, commonly used for pain and inflammation, may have altered absorption in individuals with celiac disease. Certain Anticonvulsants: Medications used to treat seizures, such as phenytoin, might be impacted by malabsorption in untreated celiac disease. Oral Contraceptives: Birth control pills, which are taken orally, may be affected by malabsorption in individuals with celiac disease. Blood Pressure Medications: Calcium Channel Blockers: Medications like amlodipine, which are calcium channel blockers used to treat high blood pressure, may be affected by impaired calcium absorption. Beta-Blockers: Some beta-blockers, such as metoprolol, may have altered absorption due to malabsorption issues. Cholesterol-Lowering Medications: Statins: Medications like atorvastatin and simvastatin, commonly prescribed for managing cholesterol levels, might be impacted by malabsorption in the small intestine. Pain Medications: Opioids: Medications containing opioids, such as codeine or oxycodone, may have absorption challenges in individuals with untreated celiac disease. Diabetes Medications: Metformin: This common medication for managing diabetes may be affected by impaired absorption in individuals with celiac disease. It's important to note that individual responses to medication can vary, and the severity of malabsorption can differ among those with celiac disease. Therefore, open communication with healthcare providers is crucial to monitor medication effectiveness, adjust dosages when needed, and explore alternative treatments if necessary. Common Supplements Affected by Celiac Disease Malabsorption Here are some common supplements that may be affected by celiac disease-related malabsorption, but many more supplements might also be affected: Calcium Supplements: Calcium carbonate or citrate: Individuals with celiac disease may experience difficulty absorbing calcium, impacting bone health. Supplementing with calcium is common to address potential deficiencies. Iron Supplements: Iron sulfate or ferrous fumarate: Celiac disease can lead to iron deficiency anemia due to impaired iron absorption. Iron supplements are often recommended to address low iron levels. Vitamin D Supplements: Cholecalciferol (Vitamin D3): Malabsorption of fat-soluble vitamins, including vitamin D, can occur in celiac disease. Supplementation is often necessary to maintain adequate vitamin D levels. B Vitamins: B12 (Methylcobalamin): Deficiencies in B vitamins, particularly B12, may occur in individuals with celiac disease due to malabsorption. B12 supplements can be prescribed to address deficiencies. Folate (Folic Acid or Methylfolate): Methylfolate: Similar to B12, folic acid absorption may be compromised. Supplementing with methylfolate can be considered. Zinc Supplements: Zinc citrate or picolinate: Zinc absorption may be reduced in celiac disease. Zinc supplementation is recommended for those with zinc deficiencies. Magnesium Supplements: Magnesium citrate or glycinate: Malabsorption issues can affect magnesium levels. Supplementing with magnesium is common to address deficiencies. Omega-3 Fatty Acids: Fish Oil (EPA and DHA): Essential fatty acids may be poorly absorbed. Omega-3 supplements can help maintain a balance of these crucial fats. Summary Individuals with untreated celiac disease may experience malabsorption of various medications and supplements due to damage to the small intestine's lining. This can impact the absorption and effectiveness of certain drugs and supplements that are commonly taken or prescribed for various conditions. It's essential for individuals with celiac disease to be aware of potential interactions and work closely with their healthcare providers, including pharmacists, to ensure appropriate adjustments in medication dosage or explore alternative forms of administration when necessary.
Celiac.com 01/27/2024 - We've done many articles that cover nutrient deficiencies that are associated with untreated celiac disease, but many people do not realize that celiac disease can also lead to malabsorption of medications and supplements. Celiac disease damages the lining of the small intestine, where both nutrient and certain medication absorption takes place. This damage can result in decreased absorption of various substances, including both over the counter and prescription medications, and supplements. Medications that are taken orally and absorbed in the small intestine may be affected by malabsorption in individuals with untreated celiac disease. As a result, the effectiveness of these medications might be compromised. It's essential for individuals with celiac disease to maintain a strict gluten-free diet to allow the small intestine to heal and improve nutrient absorption, including medications. Common Medications Affected by Celiac Disease Malabsorption Here are some common medications that may be affected by celiac disease-related malabsorption, but many more medications might also be affected: Thyroid Medications: Medications used to treat thyroid disorders, such as levothyroxine, may have reduced absorption in individuals with untreated celiac disease. Certain Antibiotics: Some antibiotics, including tetracycline and doxycycline, are absorbed in the small intestine. Malabsorption issues may affect their effectiveness. Anti-Inflammatory Drugs: Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen, commonly used for pain and inflammation, may have altered absorption in individuals with celiac disease. Certain Anticonvulsants: Medications used to treat seizures, such as phenytoin, might be impacted by malabsorption in untreated celiac disease. Oral Contraceptives: Birth control pills, which are taken orally, may be affected by malabsorption in individuals with celiac disease. Blood Pressure Medications: Calcium Channel Blockers: Medications like amlodipine, which are calcium channel blockers used to treat high blood pressure, may be affected by impaired calcium absorption. Beta-Blockers: Some beta-blockers, such as metoprolol, may have altered absorption due to malabsorption issues. Cholesterol-Lowering Medications: Statins: Medications like atorvastatin and simvastatin, commonly prescribed for managing cholesterol levels, might be impacted by malabsorption in the small intestine. Pain Medications: Opioids: Medications containing opioids, such as codeine or oxycodone, may have absorption challenges in individuals with untreated celiac disease. Diabetes Medications: Metformin: This common medication for managing diabetes may be affected by impaired absorption in individuals with celiac disease. It's important to note that individual responses to medication can vary, and the severity of malabsorption can differ among those with celiac disease. Therefore, open communication with healthcare providers is crucial to monitor medication effectiveness, adjust dosages when needed, and explore alternative treatments if necessary. Common Supplements Affected by Celiac Disease Malabsorption Here are some common supplements that may be affected by celiac disease-related malabsorption, but many more supplements might also be affected: Calcium Supplements: Calcium carbonate or citrate: Individuals with celiac disease may experience difficulty absorbing calcium, impacting bone health. Supplementing with calcium is common to address potential deficiencies. Iron Supplements: Iron sulfate or ferrous fumarate: Celiac disease can lead to iron deficiency anemia due to impaired iron absorption. Iron supplements are often recommended to address low iron levels. Vitamin D Supplements: Cholecalciferol (Vitamin D3): Malabsorption of fat-soluble vitamins, including vitamin D, can occur in celiac disease. Supplementation is often necessary to maintain adequate vitamin D levels. B Vitamins: B12 (Methylcobalamin): Deficiencies in B vitamins, particularly B12, may occur in individuals with celiac disease due to malabsorption. B12 supplements can be prescribed to address deficiencies. Folate (Folic Acid or Methylfolate): Methylfolate: Similar to B12, folic acid absorption may be compromised. Supplementing with methylfolate can be considered. Zinc Supplements: Zinc citrate or picolinate: Zinc absorption may be reduced in celiac disease. Zinc supplementation is recommended for those with zinc deficiencies. Magnesium Supplements: Magnesium citrate or glycinate: Malabsorption issues can affect magnesium levels. Supplementing with magnesium is common to address deficiencies. Omega-3 Fatty Acids: Fish Oil (EPA and DHA): Essential fatty acids may be poorly absorbed. Omega-3 supplements can help maintain a balance of these crucial fats. Summary Individuals with untreated celiac disease may experience malabsorption of various medications and supplements due to damage to the small intestine's lining. This can impact the absorption and effectiveness of certain drugs and supplements that are commonly taken or prescribed for various conditions. It's essential for individuals with celiac disease to be aware of potential interactions and work closely with their healthcare providers, including pharmacists, to ensure appropriate adjustments in medication dosage or explore alternative forms of administration when necessary. -

 Celiac.com 06/06/2023 - Celiac disease, osteopenia and osteoporosis are conditions that have been found to be connected. A research team recently described celiac disease-induced osteoporosis in an attempt to enlighten new and lesser-known aspects, including the influence of the intestinal microbiome and sex-related differences, on bone health. The team included Lisa Lungaro, Francesca Manza, Anna Costanzini, Marianna Barbalinardo, Denis Gentili, Fabio Caputo, Matteo Guarino, Giorgio Zoli, Umberto Volta, Roberto De Giorgio, and Giacomo Caio. They are variously affiliated with the Department of Translational Medicine, University of Ferrara in Ferrara, Italy; the National Research Council, Institute for the Study of Nanostructured Materials (CNR-ISMN) in Bologna, Italy; the Department of Medical and Surgical Sciences, University of Bologna, in Bologna, Italy; the Mucosal Immunology and Biology Research Center, Massachusetts General Hospital—Harvard Medical School in Boston, MA, USA. Their review describes the role of celiac disease in the development of skeletal alterations, in order to provide physicians with an updated overview on this debated topic, and to improve the management of osteoporosis in celiac disease. It is important to note that not all individuals with celiac disease will develop osteoporosis. The risk varies depending on factors such as the duration and severity of the disease, adherence to a gluten-free diet, and individual variations in bone health and genetics. However, individuals with celiac disease should be aware of the increased risk of osteoporosis and take steps to manage their bone health, including ensuring adequate calcium and vitamin D intake, monitoring bone density through regular screenings, and maintaining strict adherence to a gluten-free diet. Several important connections between the conditions highlighted by the researchers include: Malabsorption Celiac disease is characterized by damage to the small intestine, leading to impaired absorption of nutrients, including calcium and vitamin D, which are essential for maintaining healthy bones. Malabsorption of these nutrients can result in reduced bone mineral density and increased risk of osteoporosis. Inflammatory Response Celiac disease triggers an immune response in the presence of gluten. This immune response involves the production of pro-inflammatory molecules, which can contribute to bone loss and increased bone turnover, leading to osteoporosis. Calcium Imbalance The malabsorption of calcium in individuals with celiac disease can disrupt the balance of calcium in the body. When there is insufficient calcium intake or absorption, the body may draw calcium from the bones, weakening them and increasing the risk of osteoporosis. Calcium intake in the young age is an essential determinant of the bone mass peak. Calcium metabolism defects are common in untreated children with celiac disease, and they return to normal with a gluten-free diet. Vitamin D Deficiency Vitamin D plays a crucial role in calcium absorption and bone health. Celiac disease can lead to reduced vitamin D absorption due to intestinal damage. Vitamin D deficiency further exacerbates the risk of osteoporosis. Gluten-Induced Autoimmunity Celiac disease is an autoimmune disorder, and individuals with autoimmune diseases, including celiac disease, have a higher risk of developing additional autoimmune conditions such as autoimmune osteoporosis. Autoimmune mechanisms may contribute to bone loss and the development of osteoporosis in individuals with celiac disease. Hormonal Imbalance Celiac disease can disrupt the endocrine system, leading to hormonal imbalances. Hormones such as estrogen and testosterone play a crucial role in maintaining bone health. Imbalances in these hormones can accelerate bone loss and increase the risk of osteoporosis. Sex Differences Women with celiac disease are at a higher risk of osteoporosis due to both indirect and direct effects. The indirect effects include factors such as early menopause and amenorrhea (absence of menstruation), which can have a negative impact on bone health. Early menopause refers to the cessation of menstruation before the age of 45, which can occur in women with celiac disease due to various factors, including hormonal imbalances and inflammation. Early menopause is concerning for bone health because estrogen, a hormone that helps maintain bone density, decreases significantly during menopause. Lower estrogen levels can accelerate bone loss and increase the risk of osteoporosis. Therefore, women with celiac disease who experience early menopause should be particularly vigilant about managing their bone health. Physicians should be aware of bone conditions linked to celiac disease that might contribute to the worsening of BMD, and should treat them promptly. There is little evidence regarding osteopenia and pharmacological osteoporosis treatment, specifically in celiac disease. Probiotic supplementation might become a novel strategy in preventing bone alterations, although the role of gut microbiota is still uncertain and not well-established yet. In the full report, the researchers offer a comprehensive dive into each of the areas mentioned above. Read more in Nutrients. 2023 Mar; 15(5): 1089 doi: 10.3390/nu15051089
Celiac.com 06/06/2023 - Celiac disease, osteopenia and osteoporosis are conditions that have been found to be connected. A research team recently described celiac disease-induced osteoporosis in an attempt to enlighten new and lesser-known aspects, including the influence of the intestinal microbiome and sex-related differences, on bone health. The team included Lisa Lungaro, Francesca Manza, Anna Costanzini, Marianna Barbalinardo, Denis Gentili, Fabio Caputo, Matteo Guarino, Giorgio Zoli, Umberto Volta, Roberto De Giorgio, and Giacomo Caio. They are variously affiliated with the Department of Translational Medicine, University of Ferrara in Ferrara, Italy; the National Research Council, Institute for the Study of Nanostructured Materials (CNR-ISMN) in Bologna, Italy; the Department of Medical and Surgical Sciences, University of Bologna, in Bologna, Italy; the Mucosal Immunology and Biology Research Center, Massachusetts General Hospital—Harvard Medical School in Boston, MA, USA. Their review describes the role of celiac disease in the development of skeletal alterations, in order to provide physicians with an updated overview on this debated topic, and to improve the management of osteoporosis in celiac disease. It is important to note that not all individuals with celiac disease will develop osteoporosis. The risk varies depending on factors such as the duration and severity of the disease, adherence to a gluten-free diet, and individual variations in bone health and genetics. However, individuals with celiac disease should be aware of the increased risk of osteoporosis and take steps to manage their bone health, including ensuring adequate calcium and vitamin D intake, monitoring bone density through regular screenings, and maintaining strict adherence to a gluten-free diet. Several important connections between the conditions highlighted by the researchers include: Malabsorption Celiac disease is characterized by damage to the small intestine, leading to impaired absorption of nutrients, including calcium and vitamin D, which are essential for maintaining healthy bones. Malabsorption of these nutrients can result in reduced bone mineral density and increased risk of osteoporosis. Inflammatory Response Celiac disease triggers an immune response in the presence of gluten. This immune response involves the production of pro-inflammatory molecules, which can contribute to bone loss and increased bone turnover, leading to osteoporosis. Calcium Imbalance The malabsorption of calcium in individuals with celiac disease can disrupt the balance of calcium in the body. When there is insufficient calcium intake or absorption, the body may draw calcium from the bones, weakening them and increasing the risk of osteoporosis. Calcium intake in the young age is an essential determinant of the bone mass peak. Calcium metabolism defects are common in untreated children with celiac disease, and they return to normal with a gluten-free diet. Vitamin D Deficiency Vitamin D plays a crucial role in calcium absorption and bone health. Celiac disease can lead to reduced vitamin D absorption due to intestinal damage. Vitamin D deficiency further exacerbates the risk of osteoporosis. Gluten-Induced Autoimmunity Celiac disease is an autoimmune disorder, and individuals with autoimmune diseases, including celiac disease, have a higher risk of developing additional autoimmune conditions such as autoimmune osteoporosis. Autoimmune mechanisms may contribute to bone loss and the development of osteoporosis in individuals with celiac disease. Hormonal Imbalance Celiac disease can disrupt the endocrine system, leading to hormonal imbalances. Hormones such as estrogen and testosterone play a crucial role in maintaining bone health. Imbalances in these hormones can accelerate bone loss and increase the risk of osteoporosis. Sex Differences Women with celiac disease are at a higher risk of osteoporosis due to both indirect and direct effects. The indirect effects include factors such as early menopause and amenorrhea (absence of menstruation), which can have a negative impact on bone health. Early menopause refers to the cessation of menstruation before the age of 45, which can occur in women with celiac disease due to various factors, including hormonal imbalances and inflammation. Early menopause is concerning for bone health because estrogen, a hormone that helps maintain bone density, decreases significantly during menopause. Lower estrogen levels can accelerate bone loss and increase the risk of osteoporosis. Therefore, women with celiac disease who experience early menopause should be particularly vigilant about managing their bone health. Physicians should be aware of bone conditions linked to celiac disease that might contribute to the worsening of BMD, and should treat them promptly. There is little evidence regarding osteopenia and pharmacological osteoporosis treatment, specifically in celiac disease. Probiotic supplementation might become a novel strategy in preventing bone alterations, although the role of gut microbiota is still uncertain and not well-established yet. In the full report, the researchers offer a comprehensive dive into each of the areas mentioned above. Read more in Nutrients. 2023 Mar; 15(5): 1089 doi: 10.3390/nu15051089- 1 comment
-
- 1
-

-
- celiac disease
- connection
- (and 4 more)
-

The Anemia and Celiac Disease Connection
Cynthia Kupper, RD, CD posted an article in Spring 2004 Issue
 Celiac.com 09/03/2022 - Anemia is one of the most common presentations in adults with newly diagnosed celiac disease. In 1996 approximately 3.4 million Americans were diagnosed with anemia, according to the Centers for Disease Control, and out of these 2.1 million were under the age of 45. Celiac disease can present with classic and/or atypical symptoms. Atypical symptoms of celiac disease are associated with malabsorption and can include iron deficiency anemia in both adults and children. Celiac disease was once thought to be a childhood disease. However the average age at diagnosis today is 40 to 50 years old. It is more commonly seen in women than men. Celiac disease is a disease that can begin in infancy with gastrointestinal symptoms, in childhood, or even late in life. Many persons diagnosed later in life may have no gastrointestinal symptoms. Often, in older adults, routine health checks discover silent celiac disease, because of undefined anemia or bone disease(3). Anemia can be a symptom of many conditions, including excess blood loss from bleeding or surgery; autoimmune diseases such as celiac disease; chronic infections, or from the use of some medications. There are different types of anemia. Blood studies are used to help determine the type of anemia, its possible cause, and the correct treatment. Macrocytic anemia is usually caused by a folate or vitamin B12 deficiency. Microcytic anemia is a caused from iron deficiency. Inflammation, either chronic or acute, can alter ferritin levels in persons with iron-deficiency anemia. When inflammation is present, iron levels can appear either normal or elevated in iron deficiency. Folate deficiency should be considered in persons who have both celiac disease and anemia. Folate is absorbed in the jejunum, the upper part of the small intestine. This is the part of the small intestine that is largely damaged in untreated or undiagnosed celiac disease. Celiac disease is a disease of malabsorption due to inflammation and damage of the microvilli and villi of the small intestine. The microvilli and villi normally increase the absorption capacity of the small intestine by expanding its surface area to nearly 500 times its length. When there is damage to the jejunum and duodenum, the absorption of many nutrients, including iron, is altered. Celiac disease is not often suspected when a person is diagnosed with persistent anemia that does not respond well to traditional therapies, even though iron absorption can be significantly altered by the damage to the intestine. Studies suggest that persons with celiac disease may present with anemia as a single symptom or one of many symptoms. The incidence of anemia in the patients with newly diagnosed celiac disease ranges from 4% in the United States, to 24% in Romania, and over 66% in East Indian patients. In surveys of members of national celiac support groups in Canada and the U.S., anemia is a common pre-celiac diagnosis. Three recent studies in the United Kingdom screened men and women with anemia for celiac disease and found undiagnosed celiac disease in 2.3 to 6.7 percent of subjects. Another study in the UK screened 1,200 people in the general population and found celiac disease in one percent, a frequency similar to that of the U.S. study. It is possible to conservatively estimate that 78,000 people with anemia in the US could have celiac disease as the cause of their anemia. Clearly, physicians treating patients with anemia should consider screening them for celiac disease, especially if the anemia is unresponsive to traditional therapy. Anemias Found in Celiac Disease Several conditions can contribute to the development of anemia, including blood loss, poor diet, genetic disorders, chronic illnesses, and damage to the bone marrow from radiation or chemotherapy. Gastrointestinal conditions, such as Crohn’s disease or celiac disease, that decrease the absorption of iron, folate, or vitamin B12 can also cause anemia. Iron-deficiency anemia is the most common type of anemia found in women. The most common causes of iron-deficiency anemia are blood loss due to menstruation or pregnancy, and poor absorption of iron from foods(15). Iron deficiency is uncommon in postmenopausal women. If iron-deficiency anemia is discovered in postmenopausal women, it is generally the result of bleeding in the gastrointestinal tract or malabsorption. Both iron-deficiency anemia and B12 deficiencies are common in celiac disease. Iron-deficiency anemia is the most common type of anemia found with celiac disease. Decreased iron and folate absorption are often seen in untreated celiac disease. Many physicians overlook iron and folate malabsorption as a cause of anemia. As part of the evaluation process for iron-deficiency anemia endoscopic procedures are often performed, generally without taking biopsies of the small intestine. If biopsies are not taken, celiac disease would be overlooked as the causal factor for the anemia. Anemia generally develops slowly with symptoms worsening over time. Common symptoms of anemia include extreme fatigue, pale skin, weakness, shortness of breath, lightheadedness, and cold hands and feet. Iron-deficiency anemia symptoms may also include with cracks at the sides of the mouth, complaints of inflamed or sore tongue, brittle nails, pica, headaches, decreased appetite, and increased infections. Some people may also experience Restless Leg Syndrome. If not treated, iron-deficiency anemia can lead to other severe health problems, such as heart irregularities; complications with premature and low-birth-weight infants; and delayed growth and development in children. Symptoms of Vitamin B12 deficiency can cause yellowing or darkening of the skin, colorblindness to yellow-blue colors, and confusion or forgetfulness. Signs of vitamin B12 deficiencies such as neurological problems, peripheral neuropathy, mental confusion and forgetfulness can be seen before anemia is diagnosed. The most likely cause of vitamin B12 deficiency in celiac disease is due to damage in the small intestine, which makes it difficult to adequately absorb B12. Bacterial overgrowth in the small intestine is another possible cause of B12 deficiency. Anemia, as a result of vitamin B12 deficiency is considered to be uncommon in celiac disease that is diagnosed early. In a small study of 39 patients, Dahele, et al., 16 (41 percent) were found to have vitamin B12 deficiency and 16 were anemic. After four months on a gluten-free diet all patients with B12 deficiency had B12 levels that normalized. Only five patients with combined folate and B12 deficiencies received B12 therapy. Dickey found in screening celiac patients with low serum vitamin B12 levels that low B12 is common in celiac disease without having pernicious anemia, and may be the only presenting manifestation of celiac disease (14). Studies by Dahele and Dickey suggest that vitamin B12 deficiency is a common condition in untreated celiac disease, however their studies do not support that pernicious anemia is associated with celiac disease. Dahele and Dickey indicate the vitamin B12 deficiency usually resolves on a gluten-free diet, without vitamin B12 replacement. Treating Anemia in Celiac Disease The most important issue in anemia as a result of celiac disease is to follow strict gluten-free diet. The small intestine must heal in order to absorb nutrients correctly and adequately. Studies indicate that it can take several months to years to heal the small intestine in persons with celiac disease, and it is imperative that all persons with celiac disease have regular follow-up visits with a dietitian to check the adequacy of their diet. A gluten-free diet alone has been shown to reverse signs of anemia in most newly diagnosed celiac patients. In otherwise healthy individuals, it takes six to 12 months of diet therapy to correct anemia. Reversing anemia in persons with celiac disease may take several months longer, even with supplementation. Iron replacement therapy may not be necessary in mildly-depleted persons. In these cases a gluten-free diet high in iron-rich foods and a good gluten-free multi-vitamin supplement should be tried for six to 12 months before further therapy options are considered. Persons taking iron supplements should take iron with vitamin C-rich foods, such as citrus juice, which will help increase iron absorption. They should also avoiding calcium and dairy products within an hour of eating iron-rich foods, as calcium binds with iron and neither nutrient is absorbed well. Iron-rich foods including fish, poultry, and red meats should be included at each meal. Use of coffee and tea should be restricted. Iron supplementation therapy recommendations for persons with celiac disease vary by physician. Recommendations of up to one gram of iron per day, with close monitoring for clinical and blood level improvement are sometimes recommended. In severe situations, blood transfusions are used to boost the patient’s initial iron and hemoglobin levels. As with other medications, all supplements used must be gluten-free. Foods rich in iron that are naturally gluten-free include: lean red meats, liver, kidney, clams, oysters, shrimp, chicken, haddock, crab, tuna, salmon, turkey, broccoli, parsley, leafy greens, peas, dried beans, lentils, peaches, pears, dates, raisins, dried prunes, and blackstrap molasses. Many of the special seeds and flours used in the gluten-free diet are rich in iron, including amaranth, buckwheat, Montina™, quinoa, and teff. These foods are also high in other nutrients, including calcium, amino acids, magnesium, zinc and fiber. When compared to whole wheat and enriched all-purpose white wheat flours (iron content 4.7 mg and 5.8 mg, respectively), many of the gluten-free flours are nutritionally equal or superior to wheat flour. Amaranth, buckwheat, flax, garfava, millet, Montina™, quinoa, rice bran and soy all have higher iron content than wheat flours. In gluten-free baking, a blend of flours is required for best results. Many of the flours mentioned above are used as secondary ingredients in the flour blends, in combination with refined starches such as rice flour, potato starch and tapioca or corn starch, all of which are much lower in iron than wheat flour. Using the whole seed or groat of these seeds in cooking can significantly increase the iron content of the gluten-free diet. Many of these products make wonderful side-dishes and starches in casseroles or soups. Teff is used as a staple food in Ethiopia. It is extremely high in iron and it is speculated that it is the extensive use of teff that keeps the incidence of iron-deficiency anemia low in Ethiopia. For persons with celiac disease who are also lactose intolerant or choose to follow a vegetarian diet, inclusion of these seeds helps to assure adequate nutrient intake. Anemia is common in the general population and even higher in celiac disease. Malabsorption is a common cause of anemia. Persons with anemia are at risk for celiac disease. Patients with anemia from unknown reasons or those who do not respond to traditional treatments require further evaluation which should include screening for celiac disease. If celiac disease is discovered, appropriate treatment with a gluten-free diet that includes foods that are rich in iron is normally all that is necessary to treat anemia in most cases. The Dietary Reference Index (RDI) for Iron: 7 to 10 mg/day for young children 8 to 11 mg/day for males 15 to 18 mg/day for females of menstrual age 8 mg/day for older females 27 mg/day during pregnancy References: Anemia, Vital and Health Statistics, Series 10, No. 200 , 1996. <http://www.cdc.gov/nchs/fastats/anemia.htm> Accessed 9/10/03 Fasano A, Berti I, et al. Prevalence of Celiac Disease in At-Risk and Not-At-Risk Groups in the United States Arch Intern Med. 2003;163:286-292. Guandalini S. Celiac disease. School Nurse News. 2003 Mar;20(2):24-7. Sood A, Midha V, et al. Adult celiac disease in northern India. Indian J Gastroenterol. 2003 Jul-Aug;22(4):124-6. Sachdev A, Srinivasan V, et al. Adult onset celiac disease in north India. Trop Gastroenterol. 2002 Jul-Sep;23(3):117-9. Dobru D, Pascu O, et al. The prevalence of coeliac disease at endoscopy units in Romania: routine biopsies during gastroscopy are mandatory (a multicentre study). Rom J Gastroenterol. 2003 Jun;12(2):97-100. Zipser RD, Patel S, et al. Presentations of adult celiac disease in a nationwide patient support group. Dig Dis Sci. 2003 Apr;48(4):761-4. Cranney A, Zarkadas M, et al. The Canadian celiac health survey – the Ottawa chapter pilot. BMC Gastroenterol. 2003; 3 (1): 8. Ransford RA, Hayes M, et al. A controlled, prospective screening study of celiac disease presenting as iron deficiency anemia. J Clin Gastroenterol. 2002 Sep;35(3):228-33. Howard MR, Turnbull AJ, et al. A prospective study of the prevalence of undiagnosed coeliac disease in laboratory defined iron and folate deficiency. J Clin Pathol. 2002 Oct;55(10):754-7. Brooklyn TN, Di Mambro AJ, et al. Patients over 45 years with iron deficiency require investigation. Eur J Gastroenterol Hepatol. 2003 May;15(5):535-8. Sanders DS, Patel D, et al. A primary care cross-sectional study of undiagnosed adult coeliac disease. Eur J Gastroenterol Hepatol. 2003 Apr;15(4):407-13. Dahele A, Ghosh S. Vitamin B12 deficiency in untreated celiac disease. Am J Gastroenterol. 2001 Mar;96(3):745-50. Dickey W. Low serum vitamin B12 is common in coeliac disease and is not due to autoimmune gastritis. Eur J Gastroenterol Hepatol. 2002 Apr;14(4):425-7. Iron-deficiency anemia in women. Harvard Women's Health Watch, Nov 2002, Vol. 10 Issue 3, p3 Anemia Patient Education Sheets. Mayo Clinic website. www.mayoclinic.org. Accessed 9-5-03. Annibale B, Severi C, et al. Efficacy of gluten-free diet alone on recovery from iron deficiency anemia in adult celiac patients. Am J Gastroenterol. 2001 Jan;96(1):132-7.
Celiac.com 09/03/2022 - Anemia is one of the most common presentations in adults with newly diagnosed celiac disease. In 1996 approximately 3.4 million Americans were diagnosed with anemia, according to the Centers for Disease Control, and out of these 2.1 million were under the age of 45. Celiac disease can present with classic and/or atypical symptoms. Atypical symptoms of celiac disease are associated with malabsorption and can include iron deficiency anemia in both adults and children. Celiac disease was once thought to be a childhood disease. However the average age at diagnosis today is 40 to 50 years old. It is more commonly seen in women than men. Celiac disease is a disease that can begin in infancy with gastrointestinal symptoms, in childhood, or even late in life. Many persons diagnosed later in life may have no gastrointestinal symptoms. Often, in older adults, routine health checks discover silent celiac disease, because of undefined anemia or bone disease(3). Anemia can be a symptom of many conditions, including excess blood loss from bleeding or surgery; autoimmune diseases such as celiac disease; chronic infections, or from the use of some medications. There are different types of anemia. Blood studies are used to help determine the type of anemia, its possible cause, and the correct treatment. Macrocytic anemia is usually caused by a folate or vitamin B12 deficiency. Microcytic anemia is a caused from iron deficiency. Inflammation, either chronic or acute, can alter ferritin levels in persons with iron-deficiency anemia. When inflammation is present, iron levels can appear either normal or elevated in iron deficiency. Folate deficiency should be considered in persons who have both celiac disease and anemia. Folate is absorbed in the jejunum, the upper part of the small intestine. This is the part of the small intestine that is largely damaged in untreated or undiagnosed celiac disease. Celiac disease is a disease of malabsorption due to inflammation and damage of the microvilli and villi of the small intestine. The microvilli and villi normally increase the absorption capacity of the small intestine by expanding its surface area to nearly 500 times its length. When there is damage to the jejunum and duodenum, the absorption of many nutrients, including iron, is altered. Celiac disease is not often suspected when a person is diagnosed with persistent anemia that does not respond well to traditional therapies, even though iron absorption can be significantly altered by the damage to the intestine. Studies suggest that persons with celiac disease may present with anemia as a single symptom or one of many symptoms. The incidence of anemia in the patients with newly diagnosed celiac disease ranges from 4% in the United States, to 24% in Romania, and over 66% in East Indian patients. In surveys of members of national celiac support groups in Canada and the U.S., anemia is a common pre-celiac diagnosis. Three recent studies in the United Kingdom screened men and women with anemia for celiac disease and found undiagnosed celiac disease in 2.3 to 6.7 percent of subjects. Another study in the UK screened 1,200 people in the general population and found celiac disease in one percent, a frequency similar to that of the U.S. study. It is possible to conservatively estimate that 78,000 people with anemia in the US could have celiac disease as the cause of their anemia. Clearly, physicians treating patients with anemia should consider screening them for celiac disease, especially if the anemia is unresponsive to traditional therapy. Anemias Found in Celiac Disease Several conditions can contribute to the development of anemia, including blood loss, poor diet, genetic disorders, chronic illnesses, and damage to the bone marrow from radiation or chemotherapy. Gastrointestinal conditions, such as Crohn’s disease or celiac disease, that decrease the absorption of iron, folate, or vitamin B12 can also cause anemia. Iron-deficiency anemia is the most common type of anemia found in women. The most common causes of iron-deficiency anemia are blood loss due to menstruation or pregnancy, and poor absorption of iron from foods(15). Iron deficiency is uncommon in postmenopausal women. If iron-deficiency anemia is discovered in postmenopausal women, it is generally the result of bleeding in the gastrointestinal tract or malabsorption. Both iron-deficiency anemia and B12 deficiencies are common in celiac disease. Iron-deficiency anemia is the most common type of anemia found with celiac disease. Decreased iron and folate absorption are often seen in untreated celiac disease. Many physicians overlook iron and folate malabsorption as a cause of anemia. As part of the evaluation process for iron-deficiency anemia endoscopic procedures are often performed, generally without taking biopsies of the small intestine. If biopsies are not taken, celiac disease would be overlooked as the causal factor for the anemia. Anemia generally develops slowly with symptoms worsening over time. Common symptoms of anemia include extreme fatigue, pale skin, weakness, shortness of breath, lightheadedness, and cold hands and feet. Iron-deficiency anemia symptoms may also include with cracks at the sides of the mouth, complaints of inflamed or sore tongue, brittle nails, pica, headaches, decreased appetite, and increased infections. Some people may also experience Restless Leg Syndrome. If not treated, iron-deficiency anemia can lead to other severe health problems, such as heart irregularities; complications with premature and low-birth-weight infants; and delayed growth and development in children. Symptoms of Vitamin B12 deficiency can cause yellowing or darkening of the skin, colorblindness to yellow-blue colors, and confusion or forgetfulness. Signs of vitamin B12 deficiencies such as neurological problems, peripheral neuropathy, mental confusion and forgetfulness can be seen before anemia is diagnosed. The most likely cause of vitamin B12 deficiency in celiac disease is due to damage in the small intestine, which makes it difficult to adequately absorb B12. Bacterial overgrowth in the small intestine is another possible cause of B12 deficiency. Anemia, as a result of vitamin B12 deficiency is considered to be uncommon in celiac disease that is diagnosed early. In a small study of 39 patients, Dahele, et al., 16 (41 percent) were found to have vitamin B12 deficiency and 16 were anemic. After four months on a gluten-free diet all patients with B12 deficiency had B12 levels that normalized. Only five patients with combined folate and B12 deficiencies received B12 therapy. Dickey found in screening celiac patients with low serum vitamin B12 levels that low B12 is common in celiac disease without having pernicious anemia, and may be the only presenting manifestation of celiac disease (14). Studies by Dahele and Dickey suggest that vitamin B12 deficiency is a common condition in untreated celiac disease, however their studies do not support that pernicious anemia is associated with celiac disease. Dahele and Dickey indicate the vitamin B12 deficiency usually resolves on a gluten-free diet, without vitamin B12 replacement. Treating Anemia in Celiac Disease The most important issue in anemia as a result of celiac disease is to follow strict gluten-free diet. The small intestine must heal in order to absorb nutrients correctly and adequately. Studies indicate that it can take several months to years to heal the small intestine in persons with celiac disease, and it is imperative that all persons with celiac disease have regular follow-up visits with a dietitian to check the adequacy of their diet. A gluten-free diet alone has been shown to reverse signs of anemia in most newly diagnosed celiac patients. In otherwise healthy individuals, it takes six to 12 months of diet therapy to correct anemia. Reversing anemia in persons with celiac disease may take several months longer, even with supplementation. Iron replacement therapy may not be necessary in mildly-depleted persons. In these cases a gluten-free diet high in iron-rich foods and a good gluten-free multi-vitamin supplement should be tried for six to 12 months before further therapy options are considered. Persons taking iron supplements should take iron with vitamin C-rich foods, such as citrus juice, which will help increase iron absorption. They should also avoiding calcium and dairy products within an hour of eating iron-rich foods, as calcium binds with iron and neither nutrient is absorbed well. Iron-rich foods including fish, poultry, and red meats should be included at each meal. Use of coffee and tea should be restricted. Iron supplementation therapy recommendations for persons with celiac disease vary by physician. Recommendations of up to one gram of iron per day, with close monitoring for clinical and blood level improvement are sometimes recommended. In severe situations, blood transfusions are used to boost the patient’s initial iron and hemoglobin levels. As with other medications, all supplements used must be gluten-free. Foods rich in iron that are naturally gluten-free include: lean red meats, liver, kidney, clams, oysters, shrimp, chicken, haddock, crab, tuna, salmon, turkey, broccoli, parsley, leafy greens, peas, dried beans, lentils, peaches, pears, dates, raisins, dried prunes, and blackstrap molasses. Many of the special seeds and flours used in the gluten-free diet are rich in iron, including amaranth, buckwheat, Montina™, quinoa, and teff. These foods are also high in other nutrients, including calcium, amino acids, magnesium, zinc and fiber. When compared to whole wheat and enriched all-purpose white wheat flours (iron content 4.7 mg and 5.8 mg, respectively), many of the gluten-free flours are nutritionally equal or superior to wheat flour. Amaranth, buckwheat, flax, garfava, millet, Montina™, quinoa, rice bran and soy all have higher iron content than wheat flours. In gluten-free baking, a blend of flours is required for best results. Many of the flours mentioned above are used as secondary ingredients in the flour blends, in combination with refined starches such as rice flour, potato starch and tapioca or corn starch, all of which are much lower in iron than wheat flour. Using the whole seed or groat of these seeds in cooking can significantly increase the iron content of the gluten-free diet. Many of these products make wonderful side-dishes and starches in casseroles or soups. Teff is used as a staple food in Ethiopia. It is extremely high in iron and it is speculated that it is the extensive use of teff that keeps the incidence of iron-deficiency anemia low in Ethiopia. For persons with celiac disease who are also lactose intolerant or choose to follow a vegetarian diet, inclusion of these seeds helps to assure adequate nutrient intake. Anemia is common in the general population and even higher in celiac disease. Malabsorption is a common cause of anemia. Persons with anemia are at risk for celiac disease. Patients with anemia from unknown reasons or those who do not respond to traditional treatments require further evaluation which should include screening for celiac disease. If celiac disease is discovered, appropriate treatment with a gluten-free diet that includes foods that are rich in iron is normally all that is necessary to treat anemia in most cases. The Dietary Reference Index (RDI) for Iron: 7 to 10 mg/day for young children 8 to 11 mg/day for males 15 to 18 mg/day for females of menstrual age 8 mg/day for older females 27 mg/day during pregnancy References: Anemia, Vital and Health Statistics, Series 10, No. 200 , 1996. <http://www.cdc.gov/nchs/fastats/anemia.htm> Accessed 9/10/03 Fasano A, Berti I, et al. Prevalence of Celiac Disease in At-Risk and Not-At-Risk Groups in the United States Arch Intern Med. 2003;163:286-292. Guandalini S. Celiac disease. School Nurse News. 2003 Mar;20(2):24-7. Sood A, Midha V, et al. Adult celiac disease in northern India. Indian J Gastroenterol. 2003 Jul-Aug;22(4):124-6. Sachdev A, Srinivasan V, et al. Adult onset celiac disease in north India. Trop Gastroenterol. 2002 Jul-Sep;23(3):117-9. Dobru D, Pascu O, et al. The prevalence of coeliac disease at endoscopy units in Romania: routine biopsies during gastroscopy are mandatory (a multicentre study). Rom J Gastroenterol. 2003 Jun;12(2):97-100. Zipser RD, Patel S, et al. Presentations of adult celiac disease in a nationwide patient support group. Dig Dis Sci. 2003 Apr;48(4):761-4. Cranney A, Zarkadas M, et al. The Canadian celiac health survey – the Ottawa chapter pilot. BMC Gastroenterol. 2003; 3 (1): 8. Ransford RA, Hayes M, et al. A controlled, prospective screening study of celiac disease presenting as iron deficiency anemia. J Clin Gastroenterol. 2002 Sep;35(3):228-33. Howard MR, Turnbull AJ, et al. A prospective study of the prevalence of undiagnosed coeliac disease in laboratory defined iron and folate deficiency. J Clin Pathol. 2002 Oct;55(10):754-7. Brooklyn TN, Di Mambro AJ, et al. Patients over 45 years with iron deficiency require investigation. Eur J Gastroenterol Hepatol. 2003 May;15(5):535-8. Sanders DS, Patel D, et al. A primary care cross-sectional study of undiagnosed adult coeliac disease. Eur J Gastroenterol Hepatol. 2003 Apr;15(4):407-13. Dahele A, Ghosh S. Vitamin B12 deficiency in untreated celiac disease. Am J Gastroenterol. 2001 Mar;96(3):745-50. Dickey W. Low serum vitamin B12 is common in coeliac disease and is not due to autoimmune gastritis. Eur J Gastroenterol Hepatol. 2002 Apr;14(4):425-7. Iron-deficiency anemia in women. Harvard Women's Health Watch, Nov 2002, Vol. 10 Issue 3, p3 Anemia Patient Education Sheets. Mayo Clinic website. www.mayoclinic.org. Accessed 9-5-03. Annibale B, Severi C, et al. Efficacy of gluten-free diet alone on recovery from iron deficiency anemia in adult celiac patients. Am J Gastroenterol. 2001 Jan;96(1):132-7.-
- 1
-
-
- anemia
- celiac disease
- (and 3 more)
-
 I have always been very very thin, since childhood My doctors have always commented about my being underweight. Unfortunately I didn't find out I had celiac until my mid 30s when I had pregnancy complications due to malabsorption. I have been gluten free almost 4 years now, and I do feel a lot better, but I am now having an even more difficult time maintaining weight. I eat more than twice what my husband does and we both eat the same meals, but he is average weight and still gains weight periodically, whereas I struggle to stay at 107 lbs at 5 ft'7 in tall. Any advice on how to gain weight ? I'm recently more disturbed about this because now that I'm not in my 20s anymore, the waif look does not Usually come with a positive reaction from people. Some of my friends have been making comments hinting that they thought that I was hiding a cancer diagnosis. Things like "You can talk to me about anything you know", "When my mother was Diagnosed with breast cancer she hid it from her friends and family for years, and it was really hard on us to find out and then have to deal with that on top of it all". Then my husband told me he overheard 1 of his coworkers saying "did you see xxx's wife?(at his company picnic)what is she on heroin?"😢 I'm so frustrated, I feel like I've tried everything and nothing works ....I don't know what to do ..... There are millions of articles talking about how to lose weight but nothing for the reverse unless you happened to be a body builder. (Yes I even tried their protein shakes etc) nothing 😭
I have always been very very thin, since childhood My doctors have always commented about my being underweight. Unfortunately I didn't find out I had celiac until my mid 30s when I had pregnancy complications due to malabsorption. I have been gluten free almost 4 years now, and I do feel a lot better, but I am now having an even more difficult time maintaining weight. I eat more than twice what my husband does and we both eat the same meals, but he is average weight and still gains weight periodically, whereas I struggle to stay at 107 lbs at 5 ft'7 in tall. Any advice on how to gain weight ? I'm recently more disturbed about this because now that I'm not in my 20s anymore, the waif look does not Usually come with a positive reaction from people. Some of my friends have been making comments hinting that they thought that I was hiding a cancer diagnosis. Things like "You can talk to me about anything you know", "When my mother was Diagnosed with breast cancer she hid it from her friends and family for years, and it was really hard on us to find out and then have to deal with that on top of it all". Then my husband told me he overheard 1 of his coworkers saying "did you see xxx's wife?(at his company picnic)what is she on heroin?"😢 I'm so frustrated, I feel like I've tried everything and nothing works ....I don't know what to do ..... There are millions of articles talking about how to lose weight but nothing for the reverse unless you happened to be a body builder. (Yes I even tried their protein shakes etc) nothing 😭 -

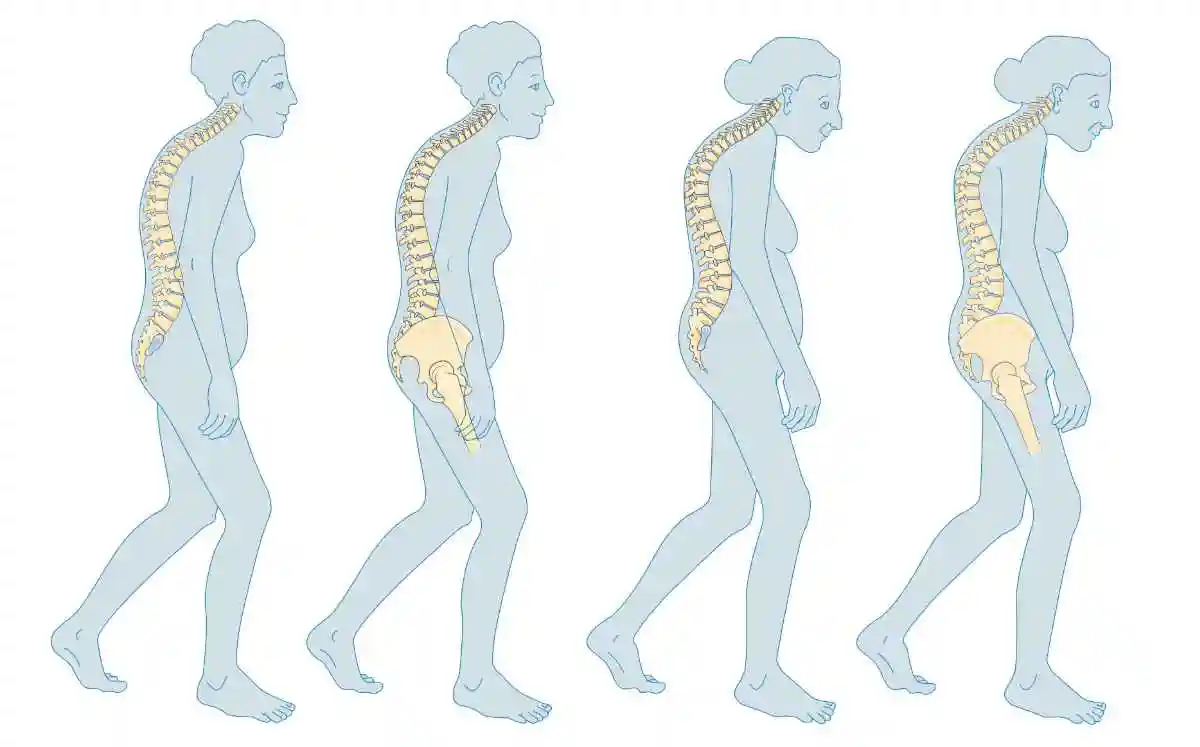
 Celiac.com 05/04/2018 - It has been recognized for several decades that both children and adults with celiac disease have a significantly increased frequency of osteoporosis and increased risk of fractures as compared to the age-matched non-celiac healthy individuals. Based on published data the prevalence of osteoporosis among celiac patients varies from as low as 4% to as high as 70%. The data from our clinic indicate that prevalence of osteoporosis among adults with gluten intolerance and celiac disease is in the vicinity of 30-40%. Characteristics and causes of osteoporosis Osteoporosis is a bone disease characterized by the reduced bone mineral density and impaired bone architecture that leads to an increased risk of fracture. The three main mechanisms by which osteoporosis develop include an inadequate peak bone mass, excessive bone resorption and inadequate formation of new bone during remodeling. At a given age, bone mass results from the amount of bone acquired during growth (the peak bone mass) minus the acquired bone loss due to variety of reasons including age-related processes, malabsorption syndromes, chronic steroid use etc. The rate and magnitude of bone mass gain during the pubertal years may markedly differ from one individual to another. It has been demonstrated that pediatric onset of celiac disease and poor compliance with gluten-free diet during childhood do significantly reduce peak bone mass. One of the main causes of osteoporosis is an alteration in bone remodeling due to imbalance between bone formation and resorption, with a predominance of resorption resulting in a reduction in bone mass and increased risk of fractures. Formation of the new bone is facilitated by specialized cells, osteoblasts, which actively synthesize bone matrix. Bone resorption is mediated by other specialized cells, osteoclasts. One of the main regulators of bone remodeling is the RANK/RANKL/OPG system. During bone remodeling, bone marrow cells and osteoblasts produce RANKL(receptor activator for nuclear factor kB ligand), which bonds with a transmembrane receptor of the osteoclast precursor, RANK(receptor activator of nuclear factor kB), causing their differentiation and activation. Osteoprotegerin (OPG) binds to RANKL before it has an opportunity to bind to RANK, and hence suppresses its ability to increase bone resorption. Normal bone remodeling is based on the permanent renovation of the skeleton and consists of an initial phase of bone resorption followed by a phase of formation, both of which are regulated by general (endocrine) factors and local (paracrine) factors. The main endocrine factors include parathyroid hormone [PTH] and vitamin D as well as estrogens and, to a lesser extent, testosterone, thyroid hormones, growth hormone and leptin. Local factors include various cytokines (IL-1, IL-6 and TNF-a playing a role) key growth factors that regulate the process. There are several well-characterized risk factors which contribute to the development of osteoporosis in celiac patients. These include: 1. Malabsorption of vitamin D and secondary hyperparathyroidism Villous atrophy in celiac patients reduces the active absorption surface and induces steatorrhea (exces fat in feces), which has a chelating effect on calcium and vitamin D, making their absorption difficult. This reduces levels of the vitamin D transporting protein (calbindin and calciumbinding protein) and increases PTH synthesis which, in turn, lead to increased bone resorption causing osteoporosis. 2. Malabsorption of vitamin K Malabsorption of fat soluble vitamins including vitamin K is a common finding in celiac patients. Three vitamin-K dependent proteins have been isolated in the bone: osteocalcin, matrix Gla protein (MGP), and protein S. Osteocalcin is a protein synthesized by osteoblasts. The synthesis of osteocalcin by osteoblasts is regulated by the active form of vitamin D—1,25-dihydroxy-cholecalciferol. The mineral-binding capacity of osteocalcin requires vitamin K-dependent gamma-carboxylation of three glutamic acid residues. MGP has been found in bone, cartilage, and soft tissue, including blood vessels. The results of animal studies suggest MGP facilitates normal bone growth and development. The vitamin K-dependent anticoagulant protein S is also synthesized by osteoblasts, but its role in bone metabolism is unclear. Children with inherited protein S deficiency suffer complications related to increased blood clotting as well as decreased bone density. The data on the role of vitamin K in osteoporosis came from the clinical observations indicating that a chronic use of vitamin K antagonists such as warfarin increases risk of vertebral and rib fractures. Accordingly, vitamin K supplementation significantly lowers risk of vertebral and hip fractures. 3. Magnesium deficiency Magnesium deficiency may be an additional risk factor for celiac-associated osteoporosis. This may be due to the fact that magnesium deficiency alters calcium metabolism and the hormones that regulate calcium. Several human studies have suggested that magnesium supplementation may improve bone mineral density. Magnesium deficiency is easily detected with laboratory tests (eg, low serum magnesium, low serum calcium, resistance to vitamin D) or clinical symptoms (eg, muscle twitching, muscle cramps, high blood pressure, irregular heartbeat). Screening for magnesium deficiency should be routinely included in the screening of celiac patients with osteoporosis. 4. Chronic diarrhea and metabolic acidosis Chronic diarrhea in patients with celiac disease results in significant bicarbonate losses and development of metabolic acidosis. Bone is a major site for the extracellular buffering of the retained acid. Therefore, one of the main compensatory mechanisms maintaining a stable serum bicarbonate level in the face of an uncorrected metabolic acidosis is the dissolution of bone buffers and net efflux of calcium from bone. Bicarbonate supplementation in patients with metabolic acidosis decreases urinary calcium, phosphorus and hydroxyproline wasting supporting the concept of negative effects of acidosis on bone health. 5. Hypogonadism Decline of estrogen production and activity is one of the main events in the development of age-related osteoporosis. It is well known that estrogen deficiency is important in the pathogenesis of osteoporosis not only in women but also in men. Increase in bone mineral density in young men and declines in older men are related to circulating free estrogen, not testosterone. In general, patients with celiac disease are characterized by low levels of circulating estrogens which contributes to the development of premature osteoporosis. 6. Chronic use of Proton Pump Inhibitors Proton pump inhibitors (PPIs) are one of the most widely used classes of drugs. The commonly used PPIs include such drugs as Omeprazole (brand name: Prilosec), Lansoprazole (brand name: Prevacid), Dexlansoprazole (brand names: Kapidex, Dexilant), Esomeprazole (brand name: Nexium), Pantoprazole (brand name: Protonix) and Rabeprazole (brand name: AcipHex). Chronic use of PPIs for gastroesophageal reflux disease and other related conditions has been associated with impaired calcium and magnesium absorption and increased risk of vertebral and nonvertebral fractures. 7. Chronic use of Selective Serotonin Reuptake Inhibitors Selective Serotonin Reuptake Inhibitors (SSRIs) are frequently used in celiac patients for treatment of depressive disorders. The commonly used SSRIs include such drugs as Citalopram (brand name: Celexa), Escitalopram (brand name: Lexapro), fluoxetine (brand name: Prozac), fluvoxamine (brand name: Luvox), Paroxetine (brand name: Paxil) and Sertraline (brand name: Zoloft). It has been demonstrated that SSRIs increase extracellular 5-HT (5-Hydroxytryptophan) levels that have deleterious skeletal effects. The skeletal serotonergic system consists of 5-HT receptors and the 5-HT transporter (5-HTT) in osteoblasts and osteocytes. 5-HTT is a transmembrane protein targeted by SSRIs. 5-HT restrains osteoblastic activity, thus leading to bone loss. 8. Autoimmune mechanisms Autoimmune mechanisms have been long suspected as risk factors contributing to development of osteoporosis in celiac patients. Near a decade ago, it was demonstrated that sera from celiac patients with osteoporosis contains significantly high titers of antibodies against bones as compared to non-celiac osteoporotic patients. The immunostaining was localized in areas where an active mineralization process occurred and was similar to the distribution of the native bone tissue transglutaminase. Recently, it has been described that a subset of patients with celiac disease has autoantibodies to osteoprotegerin, which block the inhibitory effect of osteoprotegerin on signaling by the receptor activator of nuclear factor (NF)-kappaB (RANK), and are associated with severe osteoporosis and high bone turnover. 9. Chronic inflammation Chronic inflammatory diseases, including celiac disease, are associated with overproduction of proinflammatory cytokines such as TNF-a, interleukin(IL)-1, IL-6, IL-11, IL-15 and IL-17 among others which activate osteoclasts and accelerate bone resorption leading to osteoporosis. In conclusion, osteoporosis associated with celiac disease is not a coincidental problem. It is a consequence of disease-specific (autoantibodies to osteoprotegerin), disease-nonspecific (malabsorption of vitamin D, K and magnesium, hypogonadism, chronic inflammation, chronic diarrhea and metabolic acidosis) and jatrogenic (overuse of PPIs and SSRIs) events accelerating resorptive processes in the skeleton. Correction of the aforementioned risk factors in celiac patients can reverse the development of osteoporosis and reduce the risk of osteoporosis-associated fractures. Bibliography: Bab I, Yirmiya R. Depression, selective serotonin reuptake inhibitors, and osteoporosis. Curr Osteoporos Rep. 2010 Dec;8(4):185-91. Bianchi ML. Inflammatory bowel diseases, celiac disease, and bone. Arch Biochem Biophys. 2010 Nov 1;503(1):54-65. Ito T, Jensen RT. Association of long-term proton pump inhibitor therapy with bone fractures and effects on absorption of calcium, vitamin B12, iron, and magnesium. Curr Gastroenterol Rep. 2010 Dec;12(6):448-57. Katz S, Weinerman S. Osteoporosis and gastrointestinal disease. Gastroenterol Hepatol (N Y). 2010 Aug;6(8):506-17. Riches PL, McRorie E, Fraser WD, Determann C, van't Hof R, Ralston SH. Osteoporosis associated with neutralizing autoantibodies against osteoprotegerin. N Engl J Med. 2009 Oct 8;361(15):1459-65. Stazi AV, Trecca A, Trinti B. Osteoporosis in celiac disease and in endocrine and reproductive disorders. World J Gastroenterol. 2008 Jan 28;14(4):498-505. Sugai E, Cherñavsky A, Pedreira S, Smecuol E, Vazquez H, Niveloni S, Mazure R, Mauriro E, Rabinovich GA, Bai JC. Bone-specific antibodies in sera from patients with celiac disease: characterization and implications in osteoporosis. J Clin Immunol. 2002 Nov;22(6):353-62. Turner J, Pellerin G, Mager D. Prevalence of metabolic bone disease in children with celiac disease is independent of symptoms at diagnosis. J Pediatr Gastroenterol Nutr. 2009 Nov;49(5):589-93. Vasquez H, Mazure R, Gonzalez D, Flores D, Pedreira S, Niveloni S, Smecuol E, Mauriño E, Bai JC. Risk of fractures in celiac disease patients: a cross-sectional, case-control study. Am J Gastroenterol. 2000 Jan;95(1):183-9.
Celiac.com 05/04/2018 - It has been recognized for several decades that both children and adults with celiac disease have a significantly increased frequency of osteoporosis and increased risk of fractures as compared to the age-matched non-celiac healthy individuals. Based on published data the prevalence of osteoporosis among celiac patients varies from as low as 4% to as high as 70%. The data from our clinic indicate that prevalence of osteoporosis among adults with gluten intolerance and celiac disease is in the vicinity of 30-40%. Characteristics and causes of osteoporosis Osteoporosis is a bone disease characterized by the reduced bone mineral density and impaired bone architecture that leads to an increased risk of fracture. The three main mechanisms by which osteoporosis develop include an inadequate peak bone mass, excessive bone resorption and inadequate formation of new bone during remodeling. At a given age, bone mass results from the amount of bone acquired during growth (the peak bone mass) minus the acquired bone loss due to variety of reasons including age-related processes, malabsorption syndromes, chronic steroid use etc. The rate and magnitude of bone mass gain during the pubertal years may markedly differ from one individual to another. It has been demonstrated that pediatric onset of celiac disease and poor compliance with gluten-free diet during childhood do significantly reduce peak bone mass. One of the main causes of osteoporosis is an alteration in bone remodeling due to imbalance between bone formation and resorption, with a predominance of resorption resulting in a reduction in bone mass and increased risk of fractures. Formation of the new bone is facilitated by specialized cells, osteoblasts, which actively synthesize bone matrix. Bone resorption is mediated by other specialized cells, osteoclasts. One of the main regulators of bone remodeling is the RANK/RANKL/OPG system. During bone remodeling, bone marrow cells and osteoblasts produce RANKL(receptor activator for nuclear factor kB ligand), which bonds with a transmembrane receptor of the osteoclast precursor, RANK(receptor activator of nuclear factor kB), causing their differentiation and activation. Osteoprotegerin (OPG) binds to RANKL before it has an opportunity to bind to RANK, and hence suppresses its ability to increase bone resorption. Normal bone remodeling is based on the permanent renovation of the skeleton and consists of an initial phase of bone resorption followed by a phase of formation, both of which are regulated by general (endocrine) factors and local (paracrine) factors. The main endocrine factors include parathyroid hormone [PTH] and vitamin D as well as estrogens and, to a lesser extent, testosterone, thyroid hormones, growth hormone and leptin. Local factors include various cytokines (IL-1, IL-6 and TNF-a playing a role) key growth factors that regulate the process. There are several well-characterized risk factors which contribute to the development of osteoporosis in celiac patients. These include: 1. Malabsorption of vitamin D and secondary hyperparathyroidism Villous atrophy in celiac patients reduces the active absorption surface and induces steatorrhea (exces fat in feces), which has a chelating effect on calcium and vitamin D, making their absorption difficult. This reduces levels of the vitamin D transporting protein (calbindin and calciumbinding protein) and increases PTH synthesis which, in turn, lead to increased bone resorption causing osteoporosis. 2. Malabsorption of vitamin K Malabsorption of fat soluble vitamins including vitamin K is a common finding in celiac patients. Three vitamin-K dependent proteins have been isolated in the bone: osteocalcin, matrix Gla protein (MGP), and protein S. Osteocalcin is a protein synthesized by osteoblasts. The synthesis of osteocalcin by osteoblasts is regulated by the active form of vitamin D—1,25-dihydroxy-cholecalciferol. The mineral-binding capacity of osteocalcin requires vitamin K-dependent gamma-carboxylation of three glutamic acid residues. MGP has been found in bone, cartilage, and soft tissue, including blood vessels. The results of animal studies suggest MGP facilitates normal bone growth and development. The vitamin K-dependent anticoagulant protein S is also synthesized by osteoblasts, but its role in bone metabolism is unclear. Children with inherited protein S deficiency suffer complications related to increased blood clotting as well as decreased bone density. The data on the role of vitamin K in osteoporosis came from the clinical observations indicating that a chronic use of vitamin K antagonists such as warfarin increases risk of vertebral and rib fractures. Accordingly, vitamin K supplementation significantly lowers risk of vertebral and hip fractures. 3. Magnesium deficiency Magnesium deficiency may be an additional risk factor for celiac-associated osteoporosis. This may be due to the fact that magnesium deficiency alters calcium metabolism and the hormones that regulate calcium. Several human studies have suggested that magnesium supplementation may improve bone mineral density. Magnesium deficiency is easily detected with laboratory tests (eg, low serum magnesium, low serum calcium, resistance to vitamin D) or clinical symptoms (eg, muscle twitching, muscle cramps, high blood pressure, irregular heartbeat). Screening for magnesium deficiency should be routinely included in the screening of celiac patients with osteoporosis. 4. Chronic diarrhea and metabolic acidosis Chronic diarrhea in patients with celiac disease results in significant bicarbonate losses and development of metabolic acidosis. Bone is a major site for the extracellular buffering of the retained acid. Therefore, one of the main compensatory mechanisms maintaining a stable serum bicarbonate level in the face of an uncorrected metabolic acidosis is the dissolution of bone buffers and net efflux of calcium from bone. Bicarbonate supplementation in patients with metabolic acidosis decreases urinary calcium, phosphorus and hydroxyproline wasting supporting the concept of negative effects of acidosis on bone health. 5. Hypogonadism Decline of estrogen production and activity is one of the main events in the development of age-related osteoporosis. It is well known that estrogen deficiency is important in the pathogenesis of osteoporosis not only in women but also in men. Increase in bone mineral density in young men and declines in older men are related to circulating free estrogen, not testosterone. In general, patients with celiac disease are characterized by low levels of circulating estrogens which contributes to the development of premature osteoporosis. 6. Chronic use of Proton Pump Inhibitors Proton pump inhibitors (PPIs) are one of the most widely used classes of drugs. The commonly used PPIs include such drugs as Omeprazole (brand name: Prilosec), Lansoprazole (brand name: Prevacid), Dexlansoprazole (brand names: Kapidex, Dexilant), Esomeprazole (brand name: Nexium), Pantoprazole (brand name: Protonix) and Rabeprazole (brand name: AcipHex). Chronic use of PPIs for gastroesophageal reflux disease and other related conditions has been associated with impaired calcium and magnesium absorption and increased risk of vertebral and nonvertebral fractures. 7. Chronic use of Selective Serotonin Reuptake Inhibitors Selective Serotonin Reuptake Inhibitors (SSRIs) are frequently used in celiac patients for treatment of depressive disorders. The commonly used SSRIs include such drugs as Citalopram (brand name: Celexa), Escitalopram (brand name: Lexapro), fluoxetine (brand name: Prozac), fluvoxamine (brand name: Luvox), Paroxetine (brand name: Paxil) and Sertraline (brand name: Zoloft). It has been demonstrated that SSRIs increase extracellular 5-HT (5-Hydroxytryptophan) levels that have deleterious skeletal effects. The skeletal serotonergic system consists of 5-HT receptors and the 5-HT transporter (5-HTT) in osteoblasts and osteocytes. 5-HTT is a transmembrane protein targeted by SSRIs. 5-HT restrains osteoblastic activity, thus leading to bone loss. 8. Autoimmune mechanisms Autoimmune mechanisms have been long suspected as risk factors contributing to development of osteoporosis in celiac patients. Near a decade ago, it was demonstrated that sera from celiac patients with osteoporosis contains significantly high titers of antibodies against bones as compared to non-celiac osteoporotic patients. The immunostaining was localized in areas where an active mineralization process occurred and was similar to the distribution of the native bone tissue transglutaminase. Recently, it has been described that a subset of patients with celiac disease has autoantibodies to osteoprotegerin, which block the inhibitory effect of osteoprotegerin on signaling by the receptor activator of nuclear factor (NF)-kappaB (RANK), and are associated with severe osteoporosis and high bone turnover. 9. Chronic inflammation Chronic inflammatory diseases, including celiac disease, are associated with overproduction of proinflammatory cytokines such as TNF-a, interleukin(IL)-1, IL-6, IL-11, IL-15 and IL-17 among others which activate osteoclasts and accelerate bone resorption leading to osteoporosis. In conclusion, osteoporosis associated with celiac disease is not a coincidental problem. It is a consequence of disease-specific (autoantibodies to osteoprotegerin), disease-nonspecific (malabsorption of vitamin D, K and magnesium, hypogonadism, chronic inflammation, chronic diarrhea and metabolic acidosis) and jatrogenic (overuse of PPIs and SSRIs) events accelerating resorptive processes in the skeleton. Correction of the aforementioned risk factors in celiac patients can reverse the development of osteoporosis and reduce the risk of osteoporosis-associated fractures. Bibliography: Bab I, Yirmiya R. Depression, selective serotonin reuptake inhibitors, and osteoporosis. Curr Osteoporos Rep. 2010 Dec;8(4):185-91. Bianchi ML. Inflammatory bowel diseases, celiac disease, and bone. Arch Biochem Biophys. 2010 Nov 1;503(1):54-65. Ito T, Jensen RT. Association of long-term proton pump inhibitor therapy with bone fractures and effects on absorption of calcium, vitamin B12, iron, and magnesium. Curr Gastroenterol Rep. 2010 Dec;12(6):448-57. Katz S, Weinerman S. Osteoporosis and gastrointestinal disease. Gastroenterol Hepatol (N Y). 2010 Aug;6(8):506-17. Riches PL, McRorie E, Fraser WD, Determann C, van't Hof R, Ralston SH. Osteoporosis associated with neutralizing autoantibodies against osteoprotegerin. N Engl J Med. 2009 Oct 8;361(15):1459-65. Stazi AV, Trecca A, Trinti B. Osteoporosis in celiac disease and in endocrine and reproductive disorders. World J Gastroenterol. 2008 Jan 28;14(4):498-505. Sugai E, Cherñavsky A, Pedreira S, Smecuol E, Vazquez H, Niveloni S, Mazure R, Mauriro E, Rabinovich GA, Bai JC. Bone-specific antibodies in sera from patients with celiac disease: characterization and implications in osteoporosis. J Clin Immunol. 2002 Nov;22(6):353-62. Turner J, Pellerin G, Mager D. Prevalence of metabolic bone disease in children with celiac disease is independent of symptoms at diagnosis. J Pediatr Gastroenterol Nutr. 2009 Nov;49(5):589-93. Vasquez H, Mazure R, Gonzalez D, Flores D, Pedreira S, Niveloni S, Smecuol E, Mauriño E, Bai JC. Risk of fractures in celiac disease patients: a cross-sectional, case-control study. Am J Gastroenterol. 2000 Jan;95(1):183-9. -
 Celiac.com 05/17/2019 (Originally published 10/08/2010) - There are many ways in which the immune system is compromised in the context of celiac disease. A lack of fats (due to fat malabsorption) can limit production of eicosanoids and other fat-dependent immune system components. Malabsorption of minerals such as zinc, copper, iron, selenium, or magnesium can also impair immune function in several ways. Malabsorption of non-metalic elements such as iodine can also impair our immune function through impairing T cell production by the thymus. The leaky gut, a chronic feature of untreated celiac disease can induce autoimmunity and deplete the very resources that protect us from infection and toxic agents. The recent successes of Larazotide are highly suggestive that it is the leaky gut that is at the very root of celiac disease, since many celiacs can consume gluten with little harm when taking this drug. Malabsorption Our cells can make use of three separate sources of energy. They can burn glucose, from carbohydrates, amino acids, from proteins, or fats which can be saturated, monounsaturated, or polyunsaturated fats. Any or all of these can be used for fuel at the cellular level. Celiac disease has long been characterized as a condition of fat malabsorption, and some fats are essential to our survival and wellness. Stephen Cunnane makes an excellent case for these essential fats in his book about the evolution of the human brain titled “Survival of the Fattest”. He shows that the human brain cannot develop normally without adequate supplies of omega 3 fatty acids. We also need fats to make many elements of the immune system. We must consume and absorb omega 3 and omega 6 fatty acids because our bodies are unable to efficiently produce them. Similarly, as our understanding has expanded, we have come to recognize that absorption of other nutrients such as minerals can also be compromised in untreated celiac disease. (Some people with celiac disease continue to battle mineral malabsorption for many years after adopting the gluten-free diet.) Patients with iron deficiency that does not respond to supplementation should be investigated for celiac disease, as refractory iron deficiency is common in untreated celiac disease (1). Iron is an important constituent of immune function and Stephen J. Oppenheimer has identified seven separate dynamics through which iron deficiency can compromise immune function. These include: Reduced neutrophil function which can be reversed through iron supplementation; Reduced numbers of T-lymphocytes; Reduced T-lymphocyte responsiveness; Impaired natural killer cell activity; Impaired interleukin 2 production; Altered macrophage migration; Altered cutaneous hypersensitivity (2). Magnesium deficiency, in the context of celiac disease, has been identified as a factor in damage to the parathyroid gland and consequent bone demineralization. Rude et al have shown that magnesium supplementation alone will reverse this problem (3). Similarly, mineral malabsorption may impede our supplies of zinc, copper, and selenium, each of which may have a negative impact on the immune system. Even a mild zinc deficiency can impair T cells, interfere with hormonal regulation of the thymus, and activation of tumor necrosis factor and natural killer cells (4). I have previously reported that natural killer cells are the body’s first line of defense against malignancy (5). Natural killer cells also help to protect us from a variety of infectious agents. Malabsorption of non-metallic elements such as iodine can also impair immune function. Not only does the thyroid gland require iodine to function properly, the healthy thymus gland contains large reserves of iodine and a wide range of immune functions require iodine. The antibacterial uses of iodine have a long history and this element was discovered early in the nineteenth century. Although iodine is now added to most table salts in the industrialized world deficiency continues to plague the third world causing preventable mental retardation. Failure to absorb this important nutrient can cause disturbances to many facets of the immune system and impair heat regulation through compromised thyroid function. Added problems with the thyroid gland can also come to the untreated celiac through autoimmunity induced by a process called molecular mimicry (more on this later) which is one of the means by which the leaky gut can also create havoc with the immune system. Leaky Gut Jon Meddings has characterized the gastrointestinal tract as a long tube running through our bodies that contains materials from the outside environment (6). Unlike our skin, we have only one layer of cells in the intestine that protects us from the outside world. These cells must selectively absorb nutrients from this material, while providing a protective barrier against constituents of our food that might harm us. These nutrients are absorbed through the epithelial cells and are released on the other side of the cells into the bloodstream. The leaky gut, as induced by gluten, is a state where excessive zonulin is produced in the intestinal lumen. This protein attaches to the epithelial cells that line the intestine. The epithelial cells move further apart leaving gaps between the cells, thus allowing matter to enter the bloodstream on the other side of the epithelial barrier. Depending on the size of these gaps, various toxins, infectious agents from our food, undigested and partly digested food particles, and even the friendly bacteria that inhabit our intestines may reach the bloodstream and beyond. Whether in the form of partial or complete proteins from foods, microbes from the external environment, or friendly bacteria from our intestines, once in the bloodstream our immune systems recognize these proteins as foreign. We produce antibodies to attack and destroy them. If these same proteins arrive in the circulation repeatedly, we will have elevated serum antibodies specifically sensitized to these proteins. Protein structures can contain enormously variable sequences of amino acids. Perhaps for the sake of efficiency, these selective antibodies recognize only one segment of the foreign protein structure, in the form of a single sequence of amino acids. According to the theory of molecular mimicry, this or a very similar sequence of amino acids may be found in proteins that form some of our own tissues. If we have elevated levels of antibodies that are made to attack such a string of amino acids, they will also attack self tissues. This is process results in autoimmune disease. Because it is difficult to predict what sequence of amino acids the immune system will choose, we cannot predict the specific self tissues that will be attacked by our immune systems. Nonetheless, if the theory of molecular mimicry is correct, gluten may be at the root of many forms of autoimmunity because of its impact on zonulin production. Celiac Disease vs. Gluten Sensitivity The greater hazard appears to lie with celiac disease rather than non-celiac gluten sensitivity, as celiac patients not only have to contend with all the problems that come from a leaky gut, they also have all the problems associated with malabsorption. However, Anderson et al report that people with gluten sensitivity showed a greater rate of all cause mortality as well as significantly increased rates of non-Hodgkin’s lymphoma and cancers of the digestive tract than were found among patients with celiac disease (7). These unfortunate data may be the direct result of the many physicians and other health care practitioners who consistently urge their patients to continue to consume gluten despite the clear evidence, in the form of anti-gliadin antibodies, that these patients are mounting an immune reaction against the most common food in their diet. Peter Green, professor of Medicine at Columbia University, has called for more attention to be paid to “the lesser degrees of intestinal inflammation and gluten sensitivity” (8). Sources: Farhad Zamani, Mehdi Mohamadnejad, Ramin Shakeri, Afsaneh Amiri, Safa Najafi, Seyed Meysam Alimohamadi, Seyed Mohamad Tavangar, Ardeshir Ghavamzadeh, Reza MalekzadehGluten sensitive enteropathy in patients with iron deficiency anemia of unknown originWorld J Gastroenterol 2008 December 28; 14(48): 7381-7385 Oppenheimer Stephen J, Iron and Its Relation to Immunity and Infectious Disease. The American Society for Nutritional Sciences Supplement, Journal of Nutrition. 2001;131:616S-635S. Rude RK, Olerich M. Magnesium deficiency: possible role in osteoporosis associated with gluten-sensitive enteropathy. Osteoporos Int. 1996;6(6):453-61. Prasad AS. Zinc and immunity. Mol Cell Biochem. 1998 Nov;188(1-2):63-9. Hoggan R. Considering wheat, rye, and barley proteins as aids to carcinogens. Med Hypotheses. 1997 Sep;49(3):285-8. Meddings J. National Conference, Canadian Celiac Association, Calgary, Alberta, Canada, 1999 Anderson LA, McMillan SA, Watson RGP, Monaghan P, Gavin AT, Fox C, Murray LI Malignancy and mortality in a population-based cohort of patients with coeliac disease or ‘gluten sensitivity’. World J Gastroenterol 2007 January 7; 13(1): 146-151 Green P H R, Mortality in Celiac Disease, Intestinal Inflammation, andGluten Sensitivity. JAMA. 2009;302(11):1225-1226.
Celiac.com 05/17/2019 (Originally published 10/08/2010) - There are many ways in which the immune system is compromised in the context of celiac disease. A lack of fats (due to fat malabsorption) can limit production of eicosanoids and other fat-dependent immune system components. Malabsorption of minerals such as zinc, copper, iron, selenium, or magnesium can also impair immune function in several ways. Malabsorption of non-metalic elements such as iodine can also impair our immune function through impairing T cell production by the thymus. The leaky gut, a chronic feature of untreated celiac disease can induce autoimmunity and deplete the very resources that protect us from infection and toxic agents. The recent successes of Larazotide are highly suggestive that it is the leaky gut that is at the very root of celiac disease, since many celiacs can consume gluten with little harm when taking this drug. Malabsorption Our cells can make use of three separate sources of energy. They can burn glucose, from carbohydrates, amino acids, from proteins, or fats which can be saturated, monounsaturated, or polyunsaturated fats. Any or all of these can be used for fuel at the cellular level. Celiac disease has long been characterized as a condition of fat malabsorption, and some fats are essential to our survival and wellness. Stephen Cunnane makes an excellent case for these essential fats in his book about the evolution of the human brain titled “Survival of the Fattest”. He shows that the human brain cannot develop normally without adequate supplies of omega 3 fatty acids. We also need fats to make many elements of the immune system. We must consume and absorb omega 3 and omega 6 fatty acids because our bodies are unable to efficiently produce them. Similarly, as our understanding has expanded, we have come to recognize that absorption of other nutrients such as minerals can also be compromised in untreated celiac disease. (Some people with celiac disease continue to battle mineral malabsorption for many years after adopting the gluten-free diet.) Patients with iron deficiency that does not respond to supplementation should be investigated for celiac disease, as refractory iron deficiency is common in untreated celiac disease (1). Iron is an important constituent of immune function and Stephen J. Oppenheimer has identified seven separate dynamics through which iron deficiency can compromise immune function. These include: Reduced neutrophil function which can be reversed through iron supplementation; Reduced numbers of T-lymphocytes; Reduced T-lymphocyte responsiveness; Impaired natural killer cell activity; Impaired interleukin 2 production; Altered macrophage migration; Altered cutaneous hypersensitivity (2). Magnesium deficiency, in the context of celiac disease, has been identified as a factor in damage to the parathyroid gland and consequent bone demineralization. Rude et al have shown that magnesium supplementation alone will reverse this problem (3). Similarly, mineral malabsorption may impede our supplies of zinc, copper, and selenium, each of which may have a negative impact on the immune system. Even a mild zinc deficiency can impair T cells, interfere with hormonal regulation of the thymus, and activation of tumor necrosis factor and natural killer cells (4). I have previously reported that natural killer cells are the body’s first line of defense against malignancy (5). Natural killer cells also help to protect us from a variety of infectious agents. Malabsorption of non-metallic elements such as iodine can also impair immune function. Not only does the thyroid gland require iodine to function properly, the healthy thymus gland contains large reserves of iodine and a wide range of immune functions require iodine. The antibacterial uses of iodine have a long history and this element was discovered early in the nineteenth century. Although iodine is now added to most table salts in the industrialized world deficiency continues to plague the third world causing preventable mental retardation. Failure to absorb this important nutrient can cause disturbances to many facets of the immune system and impair heat regulation through compromised thyroid function. Added problems with the thyroid gland can also come to the untreated celiac through autoimmunity induced by a process called molecular mimicry (more on this later) which is one of the means by which the leaky gut can also create havoc with the immune system. Leaky Gut Jon Meddings has characterized the gastrointestinal tract as a long tube running through our bodies that contains materials from the outside environment (6). Unlike our skin, we have only one layer of cells in the intestine that protects us from the outside world. These cells must selectively absorb nutrients from this material, while providing a protective barrier against constituents of our food that might harm us. These nutrients are absorbed through the epithelial cells and are released on the other side of the cells into the bloodstream. The leaky gut, as induced by gluten, is a state where excessive zonulin is produced in the intestinal lumen. This protein attaches to the epithelial cells that line the intestine. The epithelial cells move further apart leaving gaps between the cells, thus allowing matter to enter the bloodstream on the other side of the epithelial barrier. Depending on the size of these gaps, various toxins, infectious agents from our food, undigested and partly digested food particles, and even the friendly bacteria that inhabit our intestines may reach the bloodstream and beyond. Whether in the form of partial or complete proteins from foods, microbes from the external environment, or friendly bacteria from our intestines, once in the bloodstream our immune systems recognize these proteins as foreign. We produce antibodies to attack and destroy them. If these same proteins arrive in the circulation repeatedly, we will have elevated serum antibodies specifically sensitized to these proteins. Protein structures can contain enormously variable sequences of amino acids. Perhaps for the sake of efficiency, these selective antibodies recognize only one segment of the foreign protein structure, in the form of a single sequence of amino acids. According to the theory of molecular mimicry, this or a very similar sequence of amino acids may be found in proteins that form some of our own tissues. If we have elevated levels of antibodies that are made to attack such a string of amino acids, they will also attack self tissues. This is process results in autoimmune disease. Because it is difficult to predict what sequence of amino acids the immune system will choose, we cannot predict the specific self tissues that will be attacked by our immune systems. Nonetheless, if the theory of molecular mimicry is correct, gluten may be at the root of many forms of autoimmunity because of its impact on zonulin production. Celiac Disease vs. Gluten Sensitivity The greater hazard appears to lie with celiac disease rather than non-celiac gluten sensitivity, as celiac patients not only have to contend with all the problems that come from a leaky gut, they also have all the problems associated with malabsorption. However, Anderson et al report that people with gluten sensitivity showed a greater rate of all cause mortality as well as significantly increased rates of non-Hodgkin’s lymphoma and cancers of the digestive tract than were found among patients with celiac disease (7). These unfortunate data may be the direct result of the many physicians and other health care practitioners who consistently urge their patients to continue to consume gluten despite the clear evidence, in the form of anti-gliadin antibodies, that these patients are mounting an immune reaction against the most common food in their diet. Peter Green, professor of Medicine at Columbia University, has called for more attention to be paid to “the lesser degrees of intestinal inflammation and gluten sensitivity” (8). Sources: Farhad Zamani, Mehdi Mohamadnejad, Ramin Shakeri, Afsaneh Amiri, Safa Najafi, Seyed Meysam Alimohamadi, Seyed Mohamad Tavangar, Ardeshir Ghavamzadeh, Reza MalekzadehGluten sensitive enteropathy in patients with iron deficiency anemia of unknown originWorld J Gastroenterol 2008 December 28; 14(48): 7381-7385 Oppenheimer Stephen J, Iron and Its Relation to Immunity and Infectious Disease. The American Society for Nutritional Sciences Supplement, Journal of Nutrition. 2001;131:616S-635S. Rude RK, Olerich M. Magnesium deficiency: possible role in osteoporosis associated with gluten-sensitive enteropathy. Osteoporos Int. 1996;6(6):453-61. Prasad AS. Zinc and immunity. Mol Cell Biochem. 1998 Nov;188(1-2):63-9. Hoggan R. Considering wheat, rye, and barley proteins as aids to carcinogens. Med Hypotheses. 1997 Sep;49(3):285-8. Meddings J. National Conference, Canadian Celiac Association, Calgary, Alberta, Canada, 1999 Anderson LA, McMillan SA, Watson RGP, Monaghan P, Gavin AT, Fox C, Murray LI Malignancy and mortality in a population-based cohort of patients with coeliac disease or ‘gluten sensitivity’. World J Gastroenterol 2007 January 7; 13(1): 146-151 Green P H R, Mortality in Celiac Disease, Intestinal Inflammation, andGluten Sensitivity. JAMA. 2009;302(11):1225-1226.- 2 comments
-
- 1
-
-
- celiac disease
- gluten sensativity
- (and 2 more)
-
 Celiac.com 09/15/2016 - Some doctors and clinicians have reported cases of severe sprue-like enteropathy associated with olmesartan, but, until now, no clear demonstration of an increased risk has been documented by epidemiological studies. Now, a French nationwide observational cohort study has shown a connection between severe intestinal malabsorption and the drug olmesartan, according to results presented by a team of researchers. Olmesartan is an angiotensin II receptor antagonist which has been used for the treatment of high blood pressure. Olmesartan is also sold commercially under the name Benicar. The research team included Mickael Basson, Myriam Mezzarobba, Alain Weill, Philippe Ricordeau, Hubert Allemand, Francois Alla, and Franck Carbonnel. They are variously affiliated with the French National Health Insurance Fund, Paris, France, and the Université Paris-Sud, Assistance Publique-Hôpitaux de Paris and Gastroenterology unit, Hôpitaux Universitaires Paris Sud, Le Kremlin Bicêtre, France. The team set out to assess, in a nationwide patient cohort, the risk of hospitalization for intestinal malabsorption associated with olmesartan compared with other angiotensin receptor blockers (ARB) and ACE inhibitors (ACEIs). From the French National Health Insurance claim database, they included all adult patients initiating ARB or ACEI between 1 January 2007 and 31 December 2012, with no prior hospitalization for intestinal malabsorption, no serology testing for celiac disease, and no prescription for a gluten-free diet product. Their main endpoint was incidence of hospitalization with a discharge diagnosis of intestinal malabsorption. The team included 4,546,680 patients, for a total of 9,010,303 person-years, and observed 218 events. Compared with ACEI, the adjusted rate ratio of hospitalization with a discharge diagnosis of intestinal malabsorption was 2.49 (95% CI 1.73 to 3.57, p Average length of hospital stay for intestinal malabsorption was longer in the olmesartan group than in the other groups (p=0.02). Compared with ACEI, the adjusted rate ratio of hospitalization for celiac disease was 4.39 (95% CI 2.77 to 6.96, p<0.0001). These results show that olmesartan is assoc qiated with higher rates of hospitalization for intestinal malabsorption and celiac disease. Source: Gut. doi:10.1136/gutjnl-2015-309690
Celiac.com 09/15/2016 - Some doctors and clinicians have reported cases of severe sprue-like enteropathy associated with olmesartan, but, until now, no clear demonstration of an increased risk has been documented by epidemiological studies. Now, a French nationwide observational cohort study has shown a connection between severe intestinal malabsorption and the drug olmesartan, according to results presented by a team of researchers. Olmesartan is an angiotensin II receptor antagonist which has been used for the treatment of high blood pressure. Olmesartan is also sold commercially under the name Benicar. The research team included Mickael Basson, Myriam Mezzarobba, Alain Weill, Philippe Ricordeau, Hubert Allemand, Francois Alla, and Franck Carbonnel. They are variously affiliated with the French National Health Insurance Fund, Paris, France, and the Université Paris-Sud, Assistance Publique-Hôpitaux de Paris and Gastroenterology unit, Hôpitaux Universitaires Paris Sud, Le Kremlin Bicêtre, France. The team set out to assess, in a nationwide patient cohort, the risk of hospitalization for intestinal malabsorption associated with olmesartan compared with other angiotensin receptor blockers (ARB) and ACE inhibitors (ACEIs). From the French National Health Insurance claim database, they included all adult patients initiating ARB or ACEI between 1 January 2007 and 31 December 2012, with no prior hospitalization for intestinal malabsorption, no serology testing for celiac disease, and no prescription for a gluten-free diet product. Their main endpoint was incidence of hospitalization with a discharge diagnosis of intestinal malabsorption. The team included 4,546,680 patients, for a total of 9,010,303 person-years, and observed 218 events. Compared with ACEI, the adjusted rate ratio of hospitalization with a discharge diagnosis of intestinal malabsorption was 2.49 (95% CI 1.73 to 3.57, p Average length of hospital stay for intestinal malabsorption was longer in the olmesartan group than in the other groups (p=0.02). Compared with ACEI, the adjusted rate ratio of hospitalization for celiac disease was 4.39 (95% CI 2.77 to 6.96, p<0.0001). These results show that olmesartan is assoc qiated with higher rates of hospitalization for intestinal malabsorption and celiac disease. Source: Gut. doi:10.1136/gutjnl-2015-309690 -
Celiac.com 06/17/2015 - Refractory celiac disease type II (RCDII) and EATL (Enteropathy Associated T-cell Lymphoma) are pre-malignant complications of celiac disease. However, there is scant medical literature and data what role malnutrition and intestinal absorption may play in these conditions. With this in mind, a team of researchers set out to conduct a comprehensive assessment of nutritional status and intestinal absorption capacity of patients with RCDII and EATL, and to compare that with data of newly diagnosed celiac disease patients. The research team included N.J. Wierdsma, P. Nijeboer, M.A. de van der Schueren, M. Berkenpas, A.A. van Bodegraven, and C.J. Mulder. They are affiliated with the Department of Nutrition and Dietetics, the Department of Gastroenterology, the Celiac Centre Amsterdam, the Department of Nutrition and Dietetics at VU University Medical Centre in Amsterdam, The Netherlands; and with the Department of Internal Medicine, Gastroenterology and Geriatrics at ATRIUM-ORBIS Medical Centre, Sittard, The Netherlands. They conducted an observational study in tertiary care setting in for 24 RCDII patients, averaging 63.8 ± 8.2 years of age, 25 EATL patients averaging 62.3 ± 5.7 years of age, and 43 celiac disease patients averaging 45.6 ± 14.8 years of age. At diagnosis, the team evaluated anthropometry (BMI, unintentional weight loss, fat-free mass index (FFMI), handgrip strength (HGS), nutritional intake, fecal losses and Resting Energy Expenditure (REE)). They found low BMI (<18.5) more often in RCDII patients than in celiac disease or EATL patients (in 33%, 12% and 12%, respectively, p = 0.029). Also, 58% of EATL patients had unintentional weight loss greater than 10% of total weight, compared to 19% of celiac disease patients, and 39% for RCDII patients (p = 0.005/0.082). The team found energy malabsorption (below 85%) in 44% of RCDII patients, and in 33% of EATL patients, compared with 21.6% in celiac disease (NS). Fecal energy losses were higher in RCDII than in celiac disease patients (589 ± 451 vs 277 ± 137 kcal/d, p = 0.017). REE was lower than predicted, with reulst greater than 10% in 60% of RCDII, 89% of EATL, and 38% of celiac disease patients (p = 0.006). Between one third and two thirds of all patients showed Low FFMI and HGS. Patients with RCDII and EATL show far worse nutritional profiles than untreated naïve celiac disease patients at presentation. This malnutrition is at least partly due to malabsorption as well as hypermetabolism. This study shows the importance of proper diagnosis, and of nutrition in the treatment of these conditions. Source: Clin Nutr. 2015 Apr 30. pii: S0261-5614(15)00124-7. doi: 10.1016/j.clnu.2015.04.014.
-
 Celiac.com 04/27/2011 - People with microscopic enteritis have microscopic and sub-microscopic changes that are associated with symptoms of gluten sensitive enteropathy, and which lead to micronutrient deficiencies. A team of researchers recently set out to examine microscopic enteritis and the pathomechanism of malabsorption. The research team included Kamran Rostami, David Al Dulaimi, Mohammad Rostami Nejad, Vincenzo Villanacci, and Mihai Danciu. They are affiliated variously with the School of Medicine, University of Birmingham, UK, the Department of Gastroenterology, Alexander Hospital in Redditch, UK, the Nejad Research Center of Gastroenterology and Liver disease, Shaheed Beheshti University, M.C., in Tehran, Iran, the 2nd Department of Pathology, Spedali Civili, University of Brescia Italy, and the “Gr. T. Popa” University of Medicine and Pharmacy in Iasi, Romania. Signs of microscopic enteritis include subtle mucosal abnormalities with no pronounced inflammation, villous effacement, erosions or ulcerations when observed with conventional light microscopy. In cases of microscopic enteritis intraepithelial lymphocytes usually fall within the normal range <25/100 enterocytes (microenteropathy), or increased (lymphocytic enteritis). Microscopic enteritis is the driving force behind atypical forms of celiac disease, previously known as 'potential' and 'latent' celiac disease. Even when there are no major mucosal changes, systemic, microscopic inflammation is a key player in pathophysiology of micro-nutrient deficiency. Microscopic enteritis or celiac disease with milder, Marsh 0–II, enteropathy is the most common feature of atypical gluten sensitivity, while celiac disease with macroscopic enteritis, and Marsh IIa–c is less common. Importantly, and in contrast to much prevailing belief, symptom severity in celiac disease seems to be unrelated to the degrees or length of affected bowel. The microenteropathy may eventually develop into pronounced villous atrophy, but one interesting finding was that severe mucosal damage does not necessarily mean worse symptoms. People with mild symptoms can have more severe damage, while those with little or no visible damage can have more severe symptoms. The finding that nutritional deficiency can be seen in patients presenting with even submicroscopic enteropathy casts doubt on the notion that severe mucosal changes, such as villous atrophy, are the sole driver of malabsorption. In fact, more and more, systemic inflammation seems to be the main driver of nutritional deficiency in such cases. Pro-inflammatory cytokines, such as TNF, appear to act at the enterocyte level, inhibiting the uptake of micronutrients like iron and phosphate. From this, it appears that malabsorption in celiac disease is secondary to inflammation and cytokine stimulation. This might explain why some patients experience milder, 'atypical' enteropathy that acts just like full-blown celiac disease. In fact, inflammation triggered by gluten-sensitized lymphocytes and cytokine stimulation seems to drive the micronutrient deficiencies in celiac disease patients, with or without villous atrophy. This finding is supported by several studies that show malabsorption syndrome to be no worse in patients with villous atrophy than in those with microenteropathy (Marsh 0–II). This theory is further bolstered by the fact that many people suffer from non-symptomatic, silent celiac disease with villous atrophy, and mucosal lesions that persist after years of successful gluten-free treatment. Over the last few years, the only type of gluten sensitivity doctors have identified is atypical presentation with microenteropathy resulting in micronutrient deficiencies. However, the team points to recent studies by Kurppa et al., and Ludvigsson et al., that suggest simple changes can improve life quality for celiac disease patients with milder enteropathy. The researchers feel strongly that patients with milder enteropathy and positive serology may benefit from a gluten-free diet, and that autoantibodies might have a more reliable positive predictive value than histology, especially in early enteropathy. Diagnosing celiac disease in its early stages, especially with little or no mucosal damage, can be very challenging. However, new studies are paving the way toward a better understanding of gluten sensitivity with microenteropathy. As a result, more patients with microenteropathy, symptoms of micronutrient deficiency and positive serology are being presented with the possible benefits of a gluten-free diet. Source: Autoimmun Highlights (2010) 1:37–38. DOI 10.1007/s13317-010-0006-4
Celiac.com 04/27/2011 - People with microscopic enteritis have microscopic and sub-microscopic changes that are associated with symptoms of gluten sensitive enteropathy, and which lead to micronutrient deficiencies. A team of researchers recently set out to examine microscopic enteritis and the pathomechanism of malabsorption. The research team included Kamran Rostami, David Al Dulaimi, Mohammad Rostami Nejad, Vincenzo Villanacci, and Mihai Danciu. They are affiliated variously with the School of Medicine, University of Birmingham, UK, the Department of Gastroenterology, Alexander Hospital in Redditch, UK, the Nejad Research Center of Gastroenterology and Liver disease, Shaheed Beheshti University, M.C., in Tehran, Iran, the 2nd Department of Pathology, Spedali Civili, University of Brescia Italy, and the “Gr. T. Popa” University of Medicine and Pharmacy in Iasi, Romania. Signs of microscopic enteritis include subtle mucosal abnormalities with no pronounced inflammation, villous effacement, erosions or ulcerations when observed with conventional light microscopy. In cases of microscopic enteritis intraepithelial lymphocytes usually fall within the normal range <25/100 enterocytes (microenteropathy), or increased (lymphocytic enteritis). Microscopic enteritis is the driving force behind atypical forms of celiac disease, previously known as 'potential' and 'latent' celiac disease. Even when there are no major mucosal changes, systemic, microscopic inflammation is a key player in pathophysiology of micro-nutrient deficiency. Microscopic enteritis or celiac disease with milder, Marsh 0–II, enteropathy is the most common feature of atypical gluten sensitivity, while celiac disease with macroscopic enteritis, and Marsh IIa–c is less common. Importantly, and in contrast to much prevailing belief, symptom severity in celiac disease seems to be unrelated to the degrees or length of affected bowel. The microenteropathy may eventually develop into pronounced villous atrophy, but one interesting finding was that severe mucosal damage does not necessarily mean worse symptoms. People with mild symptoms can have more severe damage, while those with little or no visible damage can have more severe symptoms. The finding that nutritional deficiency can be seen in patients presenting with even submicroscopic enteropathy casts doubt on the notion that severe mucosal changes, such as villous atrophy, are the sole driver of malabsorption. In fact, more and more, systemic inflammation seems to be the main driver of nutritional deficiency in such cases. Pro-inflammatory cytokines, such as TNF, appear to act at the enterocyte level, inhibiting the uptake of micronutrients like iron and phosphate. From this, it appears that malabsorption in celiac disease is secondary to inflammation and cytokine stimulation. This might explain why some patients experience milder, 'atypical' enteropathy that acts just like full-blown celiac disease. In fact, inflammation triggered by gluten-sensitized lymphocytes and cytokine stimulation seems to drive the micronutrient deficiencies in celiac disease patients, with or without villous atrophy. This finding is supported by several studies that show malabsorption syndrome to be no worse in patients with villous atrophy than in those with microenteropathy (Marsh 0–II). This theory is further bolstered by the fact that many people suffer from non-symptomatic, silent celiac disease with villous atrophy, and mucosal lesions that persist after years of successful gluten-free treatment. Over the last few years, the only type of gluten sensitivity doctors have identified is atypical presentation with microenteropathy resulting in micronutrient deficiencies. However, the team points to recent studies by Kurppa et al., and Ludvigsson et al., that suggest simple changes can improve life quality for celiac disease patients with milder enteropathy. The researchers feel strongly that patients with milder enteropathy and positive serology may benefit from a gluten-free diet, and that autoantibodies might have a more reliable positive predictive value than histology, especially in early enteropathy. Diagnosing celiac disease in its early stages, especially with little or no mucosal damage, can be very challenging. However, new studies are paving the way toward a better understanding of gluten sensitivity with microenteropathy. As a result, more patients with microenteropathy, symptoms of micronutrient deficiency and positive serology are being presented with the possible benefits of a gluten-free diet. Source: Autoimmun Highlights (2010) 1:37–38. DOI 10.1007/s13317-010-0006-4 -
Celiac.com 05/12/2010 - Diarrhea, weight loss and malabsorption represent the major clinical presentation of celiac disease, but the exact mechanisms of these symptoms are not fully understood. A team of researchers recently set out to determine whether celiac disease impairs the function of solute transporters and aquaporins. The research team included U. Laforenza, E. Miceli, G. Gastaldi, M. F. Scaffino, U. Ventura, J. M. Fontana, M. N. Orsenigo, and G. R. Corazza. The team looked for possible alteration in the expression and localization of water channels, known as aquaporins, and certain solute transporters in duodenal mucosa of celiac disease patients. To do this, the team evaluated duodenal biopsies from untreated celiacs, treated celiacs, healthy controls and disease controls. The team used semi-quantitative RT-PCR and real time RT-PCR to determine the expression of some aquaporins and transporters mRNA in the duodenal biopsies. They relied on immunohistochemistry to evaluate the localization of aquaporin 3, 7 and 10, and of Na+/glucose cotransporter, H+/oligopeptide transporter and Na+/H+ exchanger. They found that the duodenal biopsies of healthy controls, treated celiac patients and disease controls expressed aquaporin 3, 7, 10, 11, Na+/glucose cotransporter, H+/oligopeptide transporter and Na+/H+ exchanger, cystic fibrosis transmembrane conductance regulator and Na-K-2Cl cotransporter mRNAs. Transcript expression was largely absent in the duodenal biopsies of untreated celiac disease patients, except for cystic fibrosis transmembrane conductance regulator and Na-K-2Cl cotransporter. Immunohistochemistry of healthy control subjects showed a labeling in the apical membrane of surface epithelial cells of duodenum. Immunolabeling was heavily reduced or absent in untreated celiac patients, but normal patients who had followed a gluten free diet for at least 1 year. The results of the study show that people with celiac disease have defects in their primary pathways for water and solute absorption that may play a role in the onset of malabsorption symptoms. Source: Biol Cell. 2010 Apr 26.
-
Bile Acid Malabsorption Related to Chronic Diarrhea
Scott Adams posted an article in Diagnosis, Testing & Treatment
Eur J Gastroenterol Hepatol 2000;12:541-547. (Celiac.com 07/09/2000) Researchers in Sweden released a report that shows a high number of patients with chronic diarrhea also have bile acid malabsorption. Further, steatorrhea is also common, but appears to be independent of bile acid malabsorption. Their study evaluated 94 patients with chronic diarrhea for loss of bile acids using both 75-SeHCAT and a fecal fat excretion tests. The patients also completed a symptom questionnaire before during a 7 day period before taking the 75-SeHCAT test. Dr. Kjell-Arne Ung and his colleagues from Sahlgrenska University Hospital, in Goteborg reported their finding in the the May issue of the European Journal of Gastroenterology and Hepatology. They found that mild steatorrhea was present in 50% of patients with non-organic bile acid malabsorption, and in 38% of patients with functional diarrhea. Further, low 75-SeHCAT levels alone is not an indicator or risk for steatorrhea, although some patients with severe organic disease had a concomitant malabsorption of fat and of bile acids. Dr. Ungs study also shows that severe steatorrhea was common in patients with celiac disease, even in patients with high 75-SeHCAT values. When compared with patients who had functional diarrhea, those with bile acid malabsorption had significantly more frequent and looser stools, however, abdominal pain, distension and flatulence was equal between those with bile acid malabsorption and normal bile acid absorption. In conclusion Dr. Ung and colleagues state: The high prevalence of bile acid malabsorption and the absence of specific symptoms, with the exception of frequent and liquid stools, indicates that the 75-SeHCAT test should be performed early in the investigation of patients with chronic diarrhea. -
George Von Hilsheimer, 1977 (Celiac.com 06/12/2000) A way the hypothalamic choreographer might be deranged is by malabsorption syndrome. If this suggestion is valid it directly leads to some simple therapeutic guidelines and implications for inexpensive and productive research - I suggest that malabsorption syndrome is a whole complex of metabolic disorders which interact with psychosocial stress, infection, allergies and endocrine disorders. Malabsorption is a stressor in itself... ...Malabsorption is associated with high levels of circulating adrenocortocotrophic hormone (ACTH) and with high levels of acetylcholine (ACh). ACTH and ACh are in turn associated with modes of learning which are characterized by poor habituation (the animals do not learn or unlearn well), by high levels of avoidance, by efficient escape conditioning, by neophobia and by poor instrumental conditioning. The experimental evidence suggests that children with malabsorption will often be similar in their electrophysiological and conditioning patterns to animals with lesions to the hypothalamus and to the hippocampus. (Di SantAgnese & Jones, 1962.)... ...Many authors have remarked on the similarity of the symptoms of sprue and celiac disease to schizophrenia (Dohan, 1969). Abnormal levels of hydrochloric acid in the stomach are associated with hysteria and neurosis (Hepler, 1970). The classic celiac syndrome is said to occur in about one case in every two thousand patients seen by pediatricians, and there is a similar frequency of nontropical sprue in adults. However, one authority (Hodgkin, 1973) reported seeing only one case of celiac disease and no sprue in ten years on a British National Health Service with 2500 patients. My own experience is that many physicians are reluctant to diagnose celiac disease and that the variability of its frequency as a diagnosis may be even greater than that among expert clinicians diagnosing diabetes from laboratory results (viz. from 2 to 76%. Jarrett & Keen (1976)... ...Consequences of Malabsorption: The ecology of the gut would be poor; Imbalances in blood chemistries and developmental anomalies would indicate neonatal and fetal nutritional inadequacy; The adrenal glands would be depleted; The immune system would be over reactive... ...Evidence for Malnutrition in Middle Class Delinquents Summarizing the preliminary reports reviewed above and looking at my delinquents in their light suggest that compared to other children: Delinquents are more often products of unfortunate pregnancies; They suffer more pregnancy and birth complications; They are seldom breast fed; They have more colic and other early indications of GI distress and food intolerance; They are often victims of celiac syndrome and other inborn errors of metabolism; They are early addicted to diets high in sugar and refined carbohydrates; They have poor absorption of food deficient intestinal flora, and slow transit times for food products moving through their guts; They have thiamin, pyridoxine and pantothenic acid deficiencies as neonates. These facts suggest that delinquents are at high risk for unusual CNS development, CNS damage, poor continuing synthesis of CNS amino acids and neural transmitters, and are extremely vulnerable to derangements of the immune and allergy systems... ...Criminal, felon (schizophrenics), and chronic patients had the greatest evidence of malabsorption syndrome of all the subjects, who generally evidenced malabsorption. Felon (schizophrenic) had lower hair Cu than (schizophrenic) patients who were not actively delinquent...
-
The following was sent to me from Rio de Janeiro by Dr. José Cesar da Fonseca Junqueira. If you have any questions you can e-mail him at: cjunqueira@ax.apc.org.br Rio de Janeiro - 05/27/96 - Celiac Disease. A Comparative study of two periods. Junqueira JC, Calçado AC, Percope S. 1996 Federal University of Rio de Janeiro Martagão Gesteira - Institute of Pediatrics. The aim of this study was to compare cases of celiac disease diagnosed in outpatients with malabsortion cases. The study was conducted at the Pediatric Gastroenterology Service of the Pediatric Institute Martagão Gesteira at the Federal University of Rio de Janeiro Brazil. It was done in two phases: from 1975 -1984 and from 1985 - 1994 (group 1, N=31 and group 2, N=21). Patients were selected based on the results of jejunal biopsy (group IV) and the favorable reaction to a gluten free diet. Data from the first interview (age, sex, nutritional status and prevalent symptoms) were analyzed. The number of biopsies and the level of compliance with the diet were also observed. The data collected was processed in a computer using EPI INFO 6.03 (January 1996)as software. The frequency of celiac disease over the studied years was compared with international data. There were no significant differences between the two groups in our study. However, the cases free of gastroenterological symptoms (atypical celiac disease) were not observed. The average age difference between the groups (group um X=24,39 months; group 2 X=32,03) was not statistically significant. A bigger study must be carried out to prove this theory. The analysis of nutritional status of the groups reveals the existence of severely undernourished patients. The number of biopsies and the level of compliance with diet were similar in the two groups. The decrease in the number of cases as well the increase in the age of patients were observed in group 2. These phenomena were probably due to a delayed exposure to gluten and to the expansion of the period of breast feeding. Other causes should be analyzed in a bigger research program. The conclusion of this study shows that there has been no change in the clinical features of the disease and points to the need for serological screening so that the entire spectrum of the disease can be established. Both groups had malabsorption and were very under-nourished (over 45%). One patient was diagnosed as having Diabetes Mellitus several years after and an other one is under investigation for poliarthrites. Serological investigation is not available in our country. The final conclusion is that we must have such serological screening to know the real spectrum of the disease. Adult celiac disease is not diagnosed in our country, mainly because the adult doctors do not know the full spectrum of celiac disease. Ill be presenting this work as a thesis at the University on May 29, 1996.
Celiac.com Sponsor (A8):
Celiac.com Sponsor (A8):
Celiac.com Sponsor (A8-M):

Celiac.com Sponsor (A8):
Celiac.com Sponsor (A8):
Celiac.com Sponsor (A8-M):