
Celiac.com 04/29/2026 - A recent case highlights an important medical problem that can easily confuse both patients and doctors: sometimes a medication can cause severe intestinal illness that looks very much like celiac disease. In this case, a woman in her sixties developed serious watery diarrhea, dehydration, low blood pressure, kidney injury, and major electrolyte problems. At first, the cause was not clear. Infection was considered, and she improved with hospital care. But when she restarted one of her usual blood pressure medicines, the diarrhea returned quickly and her kidney problems came back as well.
Doctors eventually identified the cause as olmesartan-induced sprue-like enteropathy, a drug reaction that can injure the small intestine and produce symptoms and biopsy findings that closely resemble celiac disease. Her symptoms improved after the medication was stopped, and she recovered without needing a gluten-free diet.
A Serious Illness That Started With Diarrhea
Celiac.com Sponsor (A12):
The woman had nearly three weeks of frequent watery diarrhea, with many bowel movements each day. By the time she reached intensive care, she was severely dehydrated and had dangerously low blood pressure. Testing showed kidney injury, acid buildup in the blood, and very low potassium. These are not minor complications. Diarrhea on this scale can quickly become life-threatening, especially in older adults.
Doctors looked for an infection, which is a common and reasonable first concern in a patient with sudden severe diarrhea. Stool testing, including checks for bacteria, viruses, and parasites, did not reveal an infectious cause. She improved with fluids, electrolyte correction, and supportive care, which made discharge seem appropriate.
But the story changed dramatically when she restarted her home medicines. Within a day, the diarrhea returned and worsened, and she had to be readmitted. That timing turned out to be the key clue.
Why the Medication Became the Main Suspect
When symptoms disappear after a drug is stopped and then return after it is restarted, doctors pay close attention. That pattern strongly suggests a medication reaction. In this case, olmesartan, a drug used to treat high blood pressure, became the leading suspect.
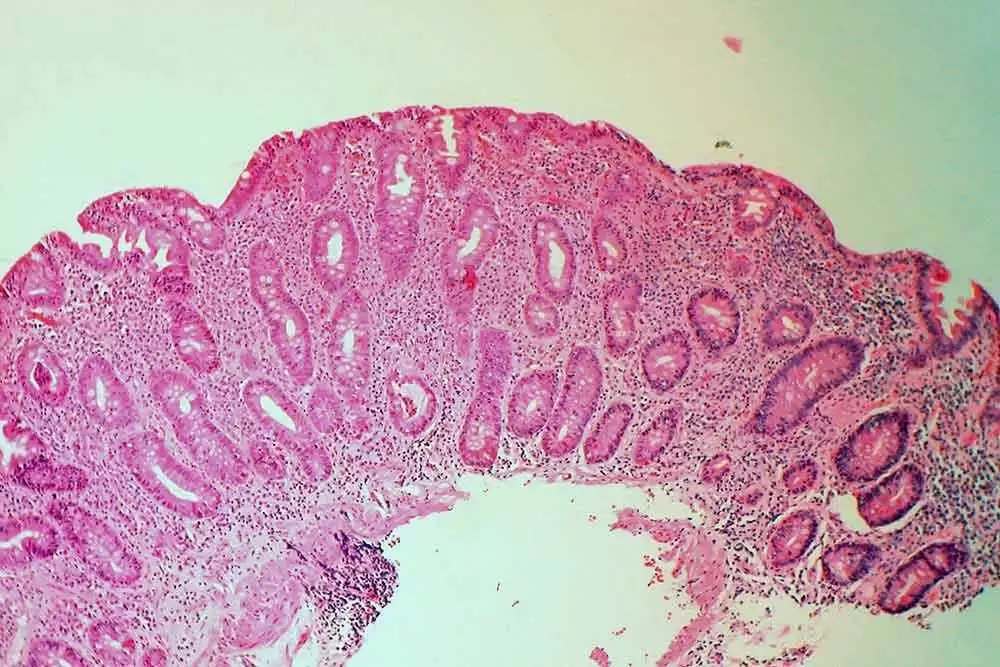
Further evaluation showed damage in the upper small intestine, including swelling, erosions, and loss of the normal villi. Those villi are tiny finger-like structures that help the body absorb nutrients. Under the microscope, the tissue also showed villous atrophy, crypt hyperplasia, and increased inflammatory immune cells. These are findings that many people in the celiac community will recognize, because they are often discussed in connection with celiac disease.
However, an important difference stood out: the woman’s blood tests for celiac disease were negative, and she got better after stopping olmesartan without making any dietary changes. That strongly supported the conclusion that the medication, not gluten, was driving the intestinal injury.
How This Can Be Confused With Celiac Disease
This is where the case becomes especially important for people with celiac disease, non-celiac gluten sensitivity, and anyone being evaluated for chronic digestive symptoms. Olmesartan-induced enteropathy can look strikingly similar to celiac disease. Patients may have severe diarrhea, weight loss, malabsorption, and intestinal damage. A biopsy may even resemble the classic pattern seen in celiac disease.
That similarity can lead to confusion. A person with drug-induced enteropathy may be told they might have celiac disease, refractory celiac disease, or a form of unexplained intestinal inflammation. If the medication is not considered as a possible cause, the true diagnosis may be delayed.
For some patients, that could mean they are incorrectly told to follow a strict gluten-free diet when the real solution is changing a prescription medicine. For others who already have celiac disease or gluten sensitivity, it could mean a new problem is wrongly blamed on accidental gluten exposure when something else is actually happening.
What Makes This Different From Celiac Disease
Celiac disease is an autoimmune condition triggered by gluten in genetically susceptible people. The core treatment is lifelong strict avoidance of gluten. When the diagnosis is correct and the diet is followed carefully, the intestine typically heals over time.
Drug-induced sprue-like enteropathy is different. The trigger is not food. The trigger is the medication. In the case described here, the patient recovered rapidly once olmesartan was discontinued. Her diarrhea resolved within forty-eight hours, and her kidney function normalized within about a week. She did not need a gluten-free diet to improve. That response helped rule out celiac disease and confirm that the drug was the main cause.
This difference matters because the treatment path is completely different. One condition requires long-term dietary treatment. The other requires removal of the offending medicine and careful selection of an alternative.
Why This Matters So Much for the Celiac Community
People with celiac disease often spend years trying to get a correct diagnosis. Many are told at first that their symptoms are stress, infection, irritable bowel syndrome, or something vague and functional. Once diagnosed, they then have to monitor foods, labels, restaurants, kitchens, and medications very carefully. Because of that, any illness that imitates celiac disease deserves serious attention.
This case matters because it shows that not every celiac-like illness is actually caused by gluten. If a patient has villous damage, diarrhea, weight loss, or malabsorption but is not improving as expected, it is important to step back and review the entire picture. That includes medications.
For patients already living gluten-free, this is especially meaningful. A person may assume their symptoms are from hidden gluten contamination when the real problem is unrelated to food. If the wrong explanation is accepted, the patient may continue suffering while making stricter and stricter dietary changes that do not solve the problem.
The Danger of Misdiagnosis
Misdiagnosis is not just frustrating. It can be dangerous. In this case, the patient became sick enough to require intensive care. Severe diarrhea can lead to dehydration, kidney injury, metabolic imbalance, weakness, dizziness, and hospitalization. If the medication had continued, the cycle might have repeated again.
There is also the emotional toll. Patients who are told they may have celiac disease often face a major life adjustment. If that diagnosis is wrong, they may spend months or years following a difficult diet unnecessarily. On the other hand, if someone really does have celiac disease but is assumed to have a medication problem alone, that can also delay appropriate treatment. The lesson is not to oversimplify. The lesson is to evaluate carefully and keep an open mind.
Questions Patients Should Ask
This case suggests several practical questions that patients with ongoing diarrhea or unexplained villous atrophy may want to discuss with their doctor. Have all current medications been reviewed as possible contributors? Did symptoms begin after a new medication was started or increased? Are celiac blood tests positive or negative? Has the intestine failed to improve despite a careful gluten-free diet? Is there a pattern of symptoms improving when a drug is stopped and returning when it is resumed?
Patients should not stop prescription medicines on their own, especially blood pressure drugs, but they should absolutely bring concerns to their medical team. A careful medication review can sometimes uncover an answer that would otherwise be missed.
What Doctors May Need to Keep in Mind
For clinicians, the case is a reminder that uncommon drug reactions can mimic common gastrointestinal diseases. If a patient has severe diarrhea, negative infectious testing, and biopsy findings that resemble celiac disease, it is reasonable to consider medication-induced enteropathy, especially if the patient is taking olmesartan. The timeline of symptom onset and recurrence after re-exposure can provide critical evidence.
The report also noted that other drugs in the same broad medication class have been linked to similar enteropathy, though olmesartan is the most recognized example. That means follow-up treatment decisions may require caution when choosing replacement blood pressure medicines.
The Bigger Message
The larger lesson is simple but powerful: intestinal injury has many causes, and even when biopsy findings resemble celiac disease, the full diagnosis still depends on context. Symptoms, blood tests, medication history, response to treatment, and follow-up all matter.
For the celiac and gluten-sensitive community, this kind of case is deeply relevant because it reinforces the need for precise diagnosis. It also validates a truth many patients already know from experience: digestive illness can be complex, and the answer is not always obvious at first.
Conclusion
This case of olmesartan-induced sprue-like enteropathy shows how a medication can create a dangerous illness that closely imitates celiac disease. The patient suffered severe diarrhea, dehydration, kidney injury, and intestinal damage, yet the true trigger was not gluten. It was a blood pressure medicine. Once the drug was stopped, she recovered quickly without changing her diet.
For people with celiac disease or gluten sensitivity, this is an important reminder that celiac-like symptoms do not always mean gluten exposure is to blame. If symptoms are severe, unusual, or persistent, a full medical review is essential. That includes a close look at prescription drugs. The better doctors and patients understand these look-alike conditions, the more likely they are to reach the right diagnosis faster and avoid unnecessary suffering.
Read more at: medscape.com












Recommended Comments
There are no comments to display.
Create an account or sign in to comment
You need to be a member in order to leave a comment
Create an account
Sign up for a new account in our community. It's easy!
Register a new accountSign in
Already have an account? Sign in here.
Sign In Now